This is a true story. Only people’s names have been changed
Mr Brown’s Story

Mr. Brown – let’s call him Jack – was lying on his back in my reception area on a bench, his wife on another chair, and I was unsure if he was quite compus mentis (mentally normal).
He stood up and his wife led as they entered my consulting rooms. They both sat down and the wife immediately started speaking on his behalf.
She briefly stated that he has been treated for cancer of the tongue but that they would like a second opinion. So I interjected, “Please go way back – start at the beginning.”
The wife started crying and the patient tried to comfort her but couldn’t speak due to pain in his tongue – a tongue that he had very little control over.
A moment late, she regained her composure and explained their situation:
Her husband – I thought it could be her father due to his worn-down appearance – noted a small lesion on the left side of his tongue.
They went to their dentist who immediately referred them to the local Oral Surgeon in the area – Dr Smith.
Dr Smith booked Jack for a procedure and excised the lesion (cut it out surgically). Dr Smith then sent the sample away to a laboratory for histological examination.
The lesion healed well, but on a follow up visit a week later they received the shocking news from Dr Smith that it was a cancerous growth.
It wasn’t all doom and gloom though. Dr Smith informed Jack that the lesion was completely removed and that it will never recur. Mr. Brown was healed. He thanked the surgeon, and the surgeon wished them well and they parted – both patient and doctor very happy at a great outcome!
The Inside Story

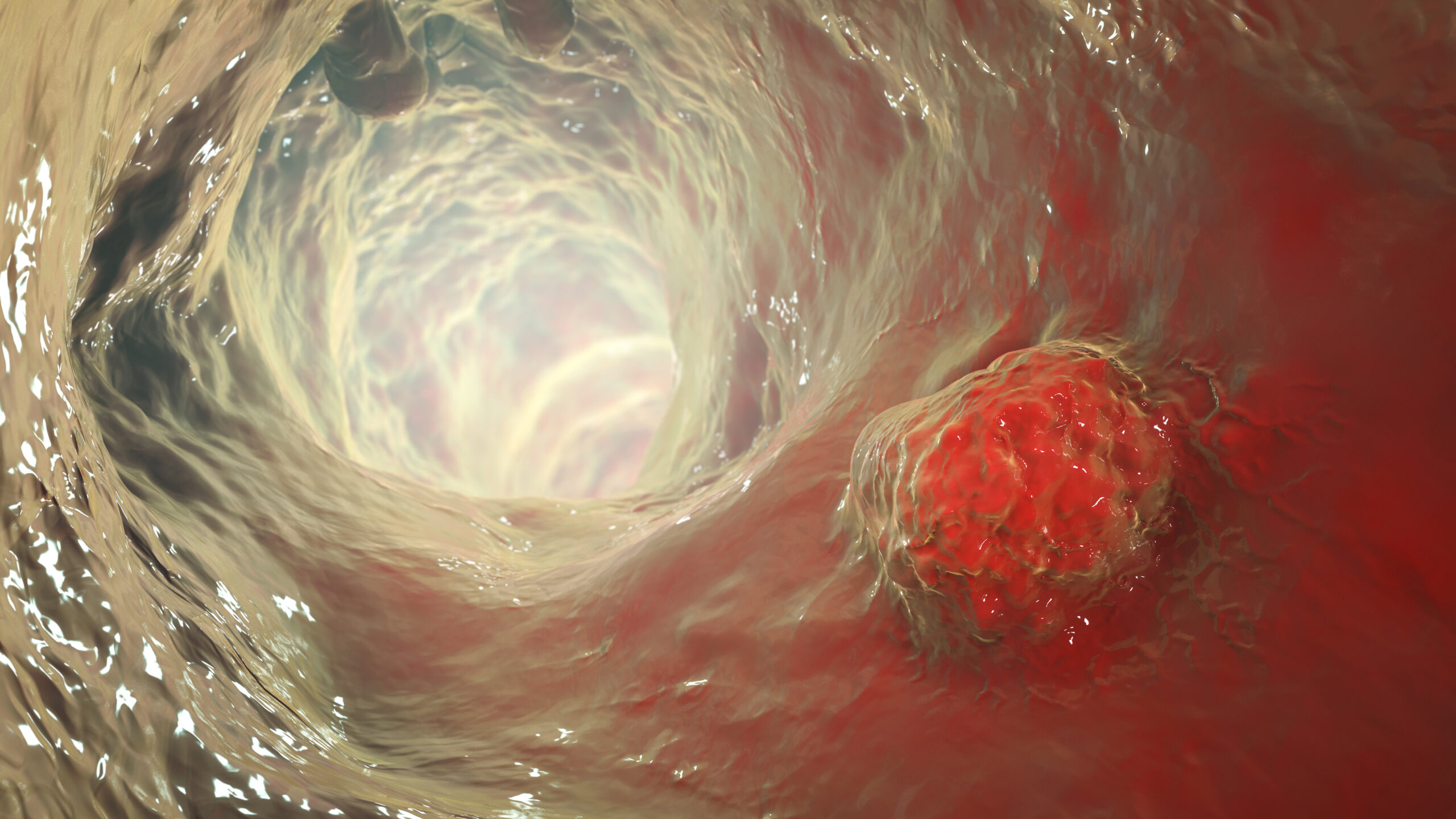
Inside Jack’s tongue, all was not well at all!
In Jack’s body, the white blood cell, commander of cancer control and extermination became very concerned. The intensity of their fight against these persistent invaders slowly but surely increased.
The problem was that it was becoming exceptionally difficult for the specialized cancer fighting units to recognize the invading cells – they were so similar to normal body cells!
There was one difference. Unlike normal tongue cells, the cancer cells divided again and again – uncontrollably and persistently!
The commander was unable to bring the state of affairs under the attention of Jack’s consciousness. This is because the specialized cancer fighting unit is part of the immune system and is being sub-contracted by the lymphatic system for the job. But the lymphatic system and the nervous system simply don’t communicate well – often not at all!
Two years later, Jack again noted a similar little ulcer in very much the same spot on his tongue.
Remembering the outcome of the previous biopsy, they promptly made an appointment at Dr Smith’s rooms – and so they met again.
Following the smiles and the Hi’s, Jack, accompanied by his very concerned wife, informed Dr Smith about the lesion.
Dr Smith examined the tongue and said that it was probably nothing more than an ulcer caused by an unintentional biting of his tongue. He prescribed an ointment and asked Mr. Brown to return in a week for a follow-up visit.
A week later the lesion hadn’t healed but looked very much the same as a week before.
So the pair went for the follow-up visit. A now very concerned patient and wife, asking numerous questions, sat in the consultation room.
Dr Smith made immediate arrangements to perform another biopsy. D?j? vu!
The story repeated almost to the letter with Dr Smith reassuring the patient and his wife: “The surgical excision margins was clear – there is nothing to worry about!” and explained that it was one of those one in a million chances that something like would happen twice in one patient – a bit like the survivor of 7 lightning strikes – a extremely rare statistical phenomenon.
A year and a bit later, one good morning, Jack thought he injured his tongue while brushing his teeth. He had a good look in the bathroom mirror, and then the concern grew during the day.
The next morning he asked his wife to have a look.
Sitting in front of Dr Smith for the third time in 5 years, Jack apparently had the same problem, again!
This time no time was wasted – an immediate biopsy – and Dr Smith promising to phone them as soon as he got the results.
Dr Smith sent the note to the histo-pathologist with a note: “URGENT” added to the referral note to pathology.
Later in the week, Jack received a phone call from Dr Smith’s receptionist, “Dr Smith wants you to please come in tomorrow morning…” and “…no I am not allowed to give results telephonically!” – in a way by saying this she gave away the diagnosis.
This time round the atmosphere was tense and the news not good. The result came back as cancer – and the lesion was incompletely removed. There were no clear margins this time.
Very clinically, and emotionally detached, Dr. Smith wrote a note to Dr Kelly – a head and neck surgeon friend of his with lots of experience in treating cancer patients.
The waiting was agony as they could only get an appointment to see Dr Kelly three weeks later. No amount of convicting or manipulation by Tracy could convince this ice cold receptionist to assist with an earlier appointment date.
The first impression of Dr Kelly was that of a well trained and very competent person – the history, the clinical examination and then the discussion. But the sentence that kept on repeating in both Jack’s and Tracey’s ears was, “I will have to surgically cut out about two thirds of your tongue?”.
Now a tongue is a wonderful organ – and one can remove a substantial amount of tongue tissue, and the tongue will recover amazingly well – increasing in size – and patients after speech therapy can talk amazingly well!
But somehow this was not communicated properly – whether Dr. Kelly didn’t spell it our well or whether emotionally perturbed patient and equally perturbed wife didn’t receive the information properly is not clear – but a critical miscommunication occurred.
Note: It is so important that one should ensure that the patient received the medical facts in a humane way – the truth – but soften it down a bit – be truthful but don’t be harsh with the facts!
The patient and wife start discussing the issues and decide that they are definitely not prepared to go for the radical tongue surgery – they cancel the appointment for surgery with Dr. Kelly and start to research the Internet for alternative options.
The world-wide-web of information in their case became a world-wide-web of misinformation. After a couple of days they came across a medical practitioner treating cancer with a special from of chemotherapy.
We all know that chemotherapy sometimes causes some nasty side-effects like hair-loss. But this practitioner used a special technique called IPT – this must be the miracle cure that they had hoped and prayed for, if the information and promises given on the website was anything to go by.
IPT is an acronym for “Insulin Potentiation Therapy”. The doctor doing the IPT was very friendly and had a ready answer for everything – even why Jack’s tongue and general condition kept on deteriorating.
It is a pity that these desperate people didn’t scroll down a bit further on the Google list for IPT – then they would have noted a serious caution about IPT by a website called “quack watch”.
Let’s read what they have to say about IPT…
Why You Should Stay Away from Insulin Potentiation Therapy by Robert Baratz, M.D., D.D.S., Ph.D.
Insulin Potentiation Therapy (IPT) is one of several unproven, dangerous treatments that is promoted by a small group of practitioners without trustworthy evidence that it works. It is claimed to be effective against cancer, infectious diseases, arthritis, and many other conditions.
After attempting this treatment and failing, eventually the couple ended up coming to me.
In front of me sat two devastated and desperate people – the man on the verge of madness by constant excruciating pain – and a woman drained to the bottom by worrying and consequent emotional breakdown.
Well time for action. Let’s do what we can do – basic principles – lets deal with the pain and sepsis as our first priority!
Orders – Admission (first, we fight with the healthcare plan to allow admission into hospital)
Hydration – Intravenous fluids, antibiotics and strong pain medication and frequent lukewarm saline mouth rinses
Consultation with a physician, a radiation oncologist and a dietitian
Arrange for X-rays and blood tests, and so the list goes on…
Off goes the precious couple to the admissions section of the hospital.
After decades of experience in clinical medicine my eyes filled with tears – Thank You God that I can still have compassion for the sick!
Thank You that my heart hasn’t hardened or gotten used to suffering!
Thank You that I can still see the man and the woman – not just another patient – and not just a source of income.
And so the story ends with an irreparable mess – the result of a number of poor clinical judgments by doctors and wrong decisions by the patient and his wife.
The best we can hope for now, based on sound scientific evidence, is palliative radiotherapy – or in simple terms, making his life as easy as possible for the next couple of years until he dies.
The radiation oncologist asked me to remove all Jack’s teeth – they were in poor condition – in preparation for the radiotherapy.
I take him to operating theater the next day, remove the teeth, and do a couple of biopsies, all confirming the diagnosis of unrestrained progressive oral cancer!
I really want to become a Doctor – Is there anything I can do straight away?




 Gloves
Gloves

 Retractors are placed strategically to help the surgical team to visualize the procedure better and to protect the adjacent important structures like the bladder.
Retractors are placed strategically to help the surgical team to visualize the procedure better and to protect the adjacent important structures like the bladder.