What is the best material to practice your suturing skills on?
Although silicon skin is helpful and convenient for the practice of suturing, it doesn’t always behave like real skin. It looks authentic, but the feel, touch and handling characteristics are imprecise if you’re looking for a genuine experience. That’s why buying high quality silicon skin is crucial if your objective is perfecting your suturing technique.
When you are preparing to start suturing on real patients in a clinical setting you want to experience some form of realism. Our philosophy and recommendation to teachers and students are simple. First master the various basic suturing patterns on a suture pad or other type of synthetic skin.
Once you have mastered your technique, go to a butcher shop or the butchery department of your grocery store and buy a suitable piece of meat with the skin attached. (Ask your butcher for advice. Pork shank, chicken or turkey with skin will serve the purpose well.) Practicing on a cut of meat is the closest approximation of human skin and muscle that you can get in a medical education setting.
Believe me – real meat from the butcher will offer you the highest level of realism possible short of suturing on real people in a clinical setting.
That said, you don’t initially need super realism to practice your suturing skills. A suture pad is more than adequate for your first practice runs. After that, strive for the most realistic option; meat from your butcher.
Master surgical suturing skills
You will find a very specific, easy and effective system of learning suturing skills in The Apprentice Doctor’sSuturing Kit and Course. Using the suturing course, you’ll master basic surgical knot tying after which you are ready to start practicing the 11 basic suturing techniques.
For those students who own some suturing tools but lack silicon skin, and find replacing cuts of meat too pricey, you may find The Apprentice Doctor’sSuture Pad/Suturing Model for Practicing Suturing an ideal compromise. Its realistic, durable design with veins, skin, fat and muscle layers is perfect for medical students, veterinarians, nurses, and emergency personal to practice and perfect suturing and laceration repair.
Both kits will allow you to become confident performing suturing procedures. You’ll feel calmer and more in control when suturing in high stress environments.
I really want to become a Doctor – Is there anything I can do straight away?
The primary goal of suturing is to approximate (bring together the wound margins) and to eliminate dead space between wound walls and edges so that underlying tissues are held together. Healing can only occur properly if the two severed areas of tissue align and remain intact. If dead space is not eliminated blood may pool in the wound leading to hematoma and consequently wound strength will be compromised, increasing the risk of infection.
The secondary goal of suturing is minimizing scar tissue formation. Both proper healing and minimal scarring are achieved by accomplishing two main objectives.
The first is ensuring that wound edges are not inverted during closure. Inversion occurs when the epidermis on either side of the wound curls inwards and touches the epidermis on the opposite side. Inversion will delay and/or compromise the healing process and leave an unsightly scar. Therefore, it is vital to proper wound healing and scar reduction to suture wounds so that edges are everted, or slightly lifted outwards.
The second objective is to achieve the best wound edge approximation. This is the process of ensuring that edges are brought together as evenly as possible during suturing. Eliminating dead space and achieving wound edge eversion and approximation are key elements for the proper healing and minimal scarring of a sutured wound.
The suture needles, materials, and techniques selected are at the discretion of the surgeon or medical professional assessing the wound. The medical professional will select the appropriate needle, suture material, and suture technique depending on whether or not they want to achieve deep tissue dead space closure, lesser or greater wound tensile strength, less scarring, ease of application or care, etc.
Keep in mind that new non-suturing closure methods are being developed that may be used as alternatives to suturing closure methods. In some situations non-suturing methods are better options than traditional suturing approaches. New methods include absorbable staples, sterile strips, and topical adhesives which can be used in combination with applied suture techniques or alone. Again, the type of suture technique or method must be determined by the treating physician or medical professional with the goal of achieving optimal wound healing and minimal scarring.
Although the use of ‘Steri-Strips’ and ‘suturing glue’ is tempting, it can only be used in very superficial wounds. Otherwise one gets a void below the surface along with associated problems like wound inversion, hematoma formation, wound infection, and wound dehiscence. It is tempting to use these shortcuts in the pediatric trauma patient, especially under the pressure that exists treating a child in the emergency room. If in doubt, suture properly under anesthetic for improved healing and an aesthetically pleasing result.
Choosing the correct suturing technique
The main driver of choice of technique in suturing is the operator’s/surgeon’s personal choice in a specific situation. He/she may gravitate to a specific technique, or combination of techniques, based on his/her knowledge, suturing proficiency, availability of specific suturing materials like suturing thread and needles, and experience gathered over the years. The medical professional will also take into account what works best in his/her hands.
No specific technique fulfills the exact requirements of a specific would closure.
Suturing Techniques – Guide (Infographic)
Suturing Techniques – Indications and Contra-indications
Here are some guidelines for the inexperienced to help you decide on which suturing technique to use.
Simple Sutures
Interrupted sutures
Interrupted sutures are sutures that are placed and tied individually. For the inexperienced this is the preferred technique due to its ability to close a wound cleanly and securely. If infection occurs in one part of the wound only a few interrupted sutures need be removed to treat the wound leaving other sutures intact. The downside is that interrupted sutures take considerably more time to place than continuous sutures.
Individual interrupted sutures also bring a limited quantity of tissue towards the closure margin – and thus in friable tissue it has a higher tendency to “pull through” when tying the knot.
It is usually not the end of the world if one interrupted suture should loosen or dehisce as the remainder of the interrupted sutures will keep the wound closed. One would not even have to replace a single interrupted suture if it loosens up so long as the resulting dehiscence is minimal and not in a critical area.
Interrupted sutures will also give a good result in curved and non-linear wounds/incisions. Unlike running sutures it will not distort the form of the wound.
Interrupted sutures offer the highest level of control over wound closure and the result. If you perceive that a specific suture is not ideally placed you can remove it and place it in a better position, unlike the running/continuous sutures where you may need to redo the entire running suture. With the interrupted suture you have excellent control over the level of wound eversion.
An unfortunate downside of using an interrupted suture is that the operator has to push the needle through healthy skin adjacent to the wound margins. This brings with it the possibility of leaving needle marks in the form of a visible row of small scars on either side (cross hatching suture marks) next to the wound margin. In esthetically sensitive areas, like the face, a surgeon will remove stitches/sutures by day 4 or 5 and secure the wound with Steri-Strips for another couple of days in an effort to avoid cross hatching scars. Do not leave interrupted facial sutures in for longer than 7 days.
Interrupted sutures with buried knots
In sensitive areas, like a tongue laceration, use the interrupted sutures with buried knots. This technique will avoid irritating the area with the 2 free ends left by a normal interrupted suture. Keep in mind that the knots may take a bit longer to resorb due to the increased amount of suture material left inside the wound. Always use absorbable sutures when using this technique.
Subcutaneous sutures
The subcutaneous suture is similar to the interrupted sutures with buried knots, but it is placed in the depth of the tissue in a surgical or traumatic wound. This suturing technique is primarily used to eliminate dead space in the depth of a wound. By default, always use absorbable sutures when using this technique
Figure-of-8 sutures
The (vertical) ‘Figure of 8 suture’ is a combination of a subcutaneous and a surface skin suture. Use this suture to save a bit of time when closing a long incision. In essence, it is a “combo-interrupted subcutaneous and skin closure suture.”
Step-by-step guide to placing simple sutures
How to Place an Interrupted Suture
How to Place an Interrupted Suture with Buried Knots
How to Place a Subcutaneous Suture
How to Place a Figure-of-8 Suture
Running (continuous) sutures
A running suture, also known as a continuous suture, consists of one strand of suture material that runs for a lengthy distance along a wound, normally in a zigzag pattern, which is tied at either end. This suture resembles those used on baseballs, and so, they are sometimes called baseball sutures. Running (continuous) sutures provide an adequate closure with even tension distribution as well as saving both time and suture material. This technique is commonly used when the wound is actively bleeding and saving time is critical, such as a scalp laceration. The disadvantage is that suture breaks can cause wound gaps to occur.
Use running sutures when esthetics are not important and when you want to save time. Running sutures tend to bunch-up the tissue and shorten the wound length due to the tension needed to keep the wound margins together. Use the running suture on an actively bleeding scalp wound when fast action is important to minimize blood loss. Since a wound of this nature is in the hairline, in most cases the cosmetic result is usually not critical.
Running sutures spread the suture tension evenly throughout the wound – and this may be important when working with tissue that has a soft consistency.
If the suture material breaks in a running suture, the whole wound will break down so be sure to secure the knots on the 2 sides and consider adding a couple of strategically placed interrupted sutures in addition to the running suture.
Continuous interlocking sutures
This suture technique is accomplished by passing the needle through the loop created by the previous suture, locking it into place. Continuous locking sutures are commonly used for breast reconstructions, intestinal surgeries, and hernias, where soft tissue requires secure stitching. The downside is when used externally on the skin permanent hatch marks may remain.
There is very little difference between regular running and interlocking running sutures. The latter tends to seal the wound margins better, which may be important in closing a wound between two cavities, e.g. closing the incision between the oral and nasal cavities following a Le Fort 1 osteotomy.
Subcuticular sutures
Apposition of the wound edge is easily achieved using the subcuticular continuous suture. Minimal scarring occurs because external sutures are not used. Rather, the subcuticular suture is applied under the epidermis using either an absorbable suture or a non-absorbable suture leaving external knots at the far ends of the laceration or incision so that the suture can be removed easily. When applied correctly, subcuticular continuous sutures provide the best outcome for cosmetic results. The drawback is that the procedure is extremely time-consuming. However, ,the sutures are easily removed, making it a common technique to use on children.
The subcuticular suture will allow for a very pleasing esthetic result in most cases, but it offers very little wound eversion by itself. Surgeons will have to get wound eversion by properly placing the subcutaneous sutures if they intend closing the surface with subcuticular sutures. One can either use absorbable or non-absorbable sutures when placing subcuticular sutures. If the choice is a thin Nylon suture remember to remove the suture within 5 days to avoid having to dissect out fragments of suture material from the semi-healed wound margin. When closing, strengthen the wound margins with Steri-Strips if needed.
Purse-string sutures
The purse-sting suture is a running suture used to close round defect wounds or openings. Predictably, the purse-string suture will not give a good cosmetic result because it will bunch-up the tissue. Purse-string sutures are typically used to close circular objects such as an areola or to close the opening after removing a chest drain (instruct the patient to take a deep breath and forcibly exhale against closed nose and lips). The suture material is passed in and out of the tissue as a running stitch and then drawn closed like closing a purse or a bag.
Step-by-step guide to placing running (continuous) sutures
How to Place Continuous (Running) Sutures
How to Place a Continuous Interlocking Suture
How to Place a Subcuticular Suture
Mattress Sutures
The 3 main reasons for using mattress sutures:
To increase the interphase or contact between the raw surface areas of two opposing wound sides.
This reason is especially important when you want to optimize the time it takes for a wound to heal, especially when one closes a fistula, such as closing an oroantral fistula (an opening between the oral and maxillary sinus cavities).
To enhance eversion.
The mattress suture provides more eversion up to the point where you may get opening of the wound edges. You may consider using the far-near suturing technique which is a variation of the vertical mattress suture.
To bring more volume or quantity of tissue to the closure area.
With a mattress suture, the chances of dehiscence are significantly reduced. However, take care not to tie mattress sutures too tightly as doing so may cause tissue strangulation and result in necrosis of the tissue on the suture-tissue contact areas.
Horizontal mattress sutures
This suturing technique is used to create moderate tension to prevent hemostasis and to improve wound tension strength for better healing. The horizontal mattress is also effective at everting wound edges and provides fair approximation. However, care must be taken to not tighten excessively or tissue ischemia can result.
Vertical mattress sutures
The vertical mattress technique is an excellent choice for achieving wound edge eversion and approximation. The technique can be used on either thin or thick skin and utilizes two bites. The first bite approximates the wound edges and the second reduces edge tension. The downside is that vertical mattress sutures can only remain in place for 5-7 days or risk is high for permanent crosshatch marks.
Near and far sutures
Also called the far-near-near-far suture or the pulley suture, this is a variation of the vertical mattress suture favored by some surgeons.
The far-and-near suture is a modified vertical mattress stitch that uses the tension created by a pulley action to close wound tissue. Because the pulley stitch reduces the surface area of large wounds in which closure cannot be accomplished completely by traditional side-to-side sutures, it is an excellent technique for areas such as the legs and scalp. Pulley sutures can be used as temporary assisting stitches, such as lessening tension for buried sutures, or they can be left in for later removal. If pulley stitches are used they must be removed promptly in order to avoid crosshatch scarring.
Step-by-step guide to placing mattress sutures
How to Place a Horizontal Mattress Suture
How to Place a Vertical Mattress Suture
How to Place Far and Near Sutures
Other suturing techniques
Ligature Sutures
This technique is used to suture tubular structures such as blood vessels in order to stop bleeding or reestablish blood flow.
Horizontal Continuous Mattress Sutures
Certain anatomical areas like the retroauricular skin, are prone to wound inversion, and this is an indication for placing horizontal continuous mattress sutures.
Horizontal Half Buried Mattress or 3-Corner Sutures
The horizontal half-buried mattress, or 3-corner suture, is used to close flapped or V-shaped wound edges. This technique is also used to better approximate edges of skin of varying texture or thickness. Also, tissue ischemia is reduced by using the 3-corner suture.
Relaxation Sutures
This suture technique is used when a wound is expected to create excessive tension. A relaxation suture allows for loosening in order to relieve such tension.
Quilting Sutures
This technique is effective at reducing the formation of seroma (swelling or lump in the underlying tissue due to serum accumulation in a localized area). A flap of skin is sutured using multiple stitches to the underlying tendinous expansion sheet (aponeurosis) that normally connects muscle tissue with its movable parts.
Retention Sutures
This technique is used to provide strong reinforcement of deep muscle and fasciae in the wall of the abdomen. Retention sutures lessen tension on the primary suture so that wound disruption is limited. The downside is that retention sutures often cause pain and severe discomfort to patients. According to one study, up to 50 percent of patients receiving retention sutures require premature removal due to complaints of pain.
Frost Sutures
This suturing technique is used during surgeries of the eyelid. Frost sutures prevent the eyelid (mainly the lower eyelid) from turning outward, known as ectropion.
Double-arm Sutures or Cobbler’s Sutures
This technique is preferred by some eye surgeons that desire to vertically or horizontally resect the rectus muscles. The double-arm suture is achieved by using a suture containing a needle at each end.
Gély’s Sutures
Similar to the double-arm suture, Gély’s suture uses suture material with a needle at both ends to close intestinal wounds. It is performed using a continuous stitch.
Czerny’s Sutures
There are two uses for Czerny’s sutures. The first involves suturing only the mucous membrane of the intestines. The second splits ruptured tendon ends and sutures the other end into the created slit much like a male/female coupling design.
Lembert Sutures
The Lembert suture is another technique used in gastrointestinal surgeries. It can be applied as either an interrupted or continuous suture that repairs the collagenous submucosal layer without disturbing the lumen.
Master Suturing Techniques Through The Apprentice Doctor!
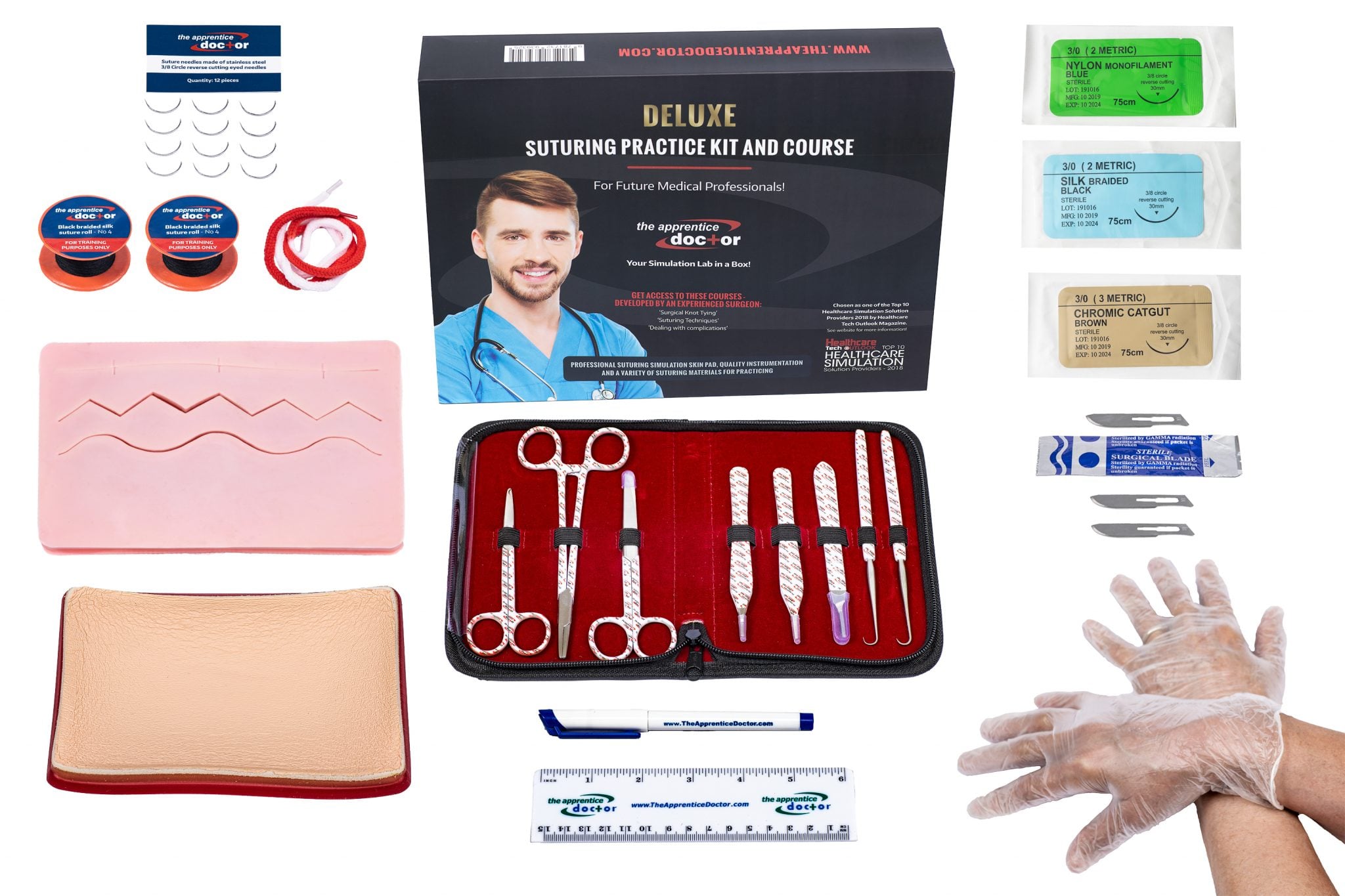
There is no need to wait on getting practice with suturing. Before you step into any situation requiring suturing, even an emergency in your own home, you can perfect your suturing skills. The Apprentice Doctor® Deluxe Suture Kit & Online Training Course teaches you how to confidently close wounds. Begin training today!
An ambulance’s siren wails as it drives up to the to the hospital’s emergency room door. Two nurses and a doctor wait as the stretcher is rolled out. The (Emergency Medicine) doctor quickly examines the patient, determines their need – and saves the person’s life.
This can be you! A doctor who daily saves lives; a person who is almost constantly in the midst of high action. Emergency medicine doctors (EMD) work in emergency rooms or trauma centers and treat patients who need immediate care. These professionals specialize in advanced cardiac life support, trauma care and management of other life-threatening conditions. [1]Emergency medicine doctors must be able to make quick decisions and lead a team of other medical professionals during intensely stressful situations. On a daily basis, EMDs…
Handle Virtually Any Emergency. Trained to handle virtually any crisis, Emergency Medical Doctors (EMD) have the tools needed to begin the management of every acute medical condition or injury that comes their way.
Make a split second/lifesaving diagnosis. Armed with quick thinking skills and a strong knowledge base, EMDs consistently make accurate decisions that save lives.
There are many advantages of being an EMD, a few of them are listed below:
See a variety of patients. EMDs see a variety of patients, including: babies and elderly patients; the critically ill and the worried well; pregnant patients and psychiatric patients. In other words, people from every walk of life.
Have a flexible schedule. EMDs typically work 8-12 hours at a time, with days off in-between. Most EMD practices do not have on-call time, which allows them to have the time to pursue outside interests.
Earn a decent salary. [3]The median salary for an EMD is $246,452. A small number of EMDs receive earning up to $500,000 or more!
The following image shows the [4]US National Average salary for EMDs:
If you are thinking of becoming an Emergency Medicine Doctor (EMD) you will face many challenges
Do you think you are up to it?
Stress level. EMDs work very hard, often managing many critical patients at one time. Some patients die in front of them. EMDs see patients who are victims of child abuse, rape, or other terrible situations.
Difficult patients. EMDs handle more “difficult” patients than most other specialties. Patients and their families are typically under strain from their acute medical conditions and therefore sometimes treat the EMD inappropriately.
To become an EMD you must have the following additional education after receiving your bachelor’s degree
Medical School: Study the major systems of the body, diseases and techniques in patient care.
Residency Program: Be introduced to the broad aspects of emergency medicine, such as critical care and trauma, and then perform rotations in specialties, such as toxicology or pediatrics.
Fellowship Program: Learn your emergency room specialty.
References
[1] https://education-portal.com/articles/ How_to_Become_an_Emergency_Medicine_Doctor_Education_Requirements_and_Career_Roadmap.html
[2] Choosing a Specialty’ Emergency Medicine: The Good, the Bad, and the Ugly; Mark Reiter, MD; Disclosures; September 30, 2011; https://www.medscape.com/viewarticle/750482
[3] MD Salaries; Emergency Medicine Physician Salary; https://mdsalaries.com/2011/08/23/emergency-medicine-physician-salary/
[5] Medscape Med Students > Choosing a Specialty’ Emergency Medicine: The Good, the Bad, and the Ugly; Mark Reiter, MD; Disclosures; September 30, 2011; https://www.medscape.com/viewarticle/750482
[6]Emergency Medicine Doctor: Educational Requirements; https://education-portal.com/articles/Emergency_Medicine_Doctor_Educational_Requirements.html
I really want to become a Doctor – Is there anything I can do straight away?
The objectives of managing a wound by suturing are obvious and simple. The first is to avoid infection from taking root in the wound. The second is to help in stopping bleeding through the wound. A third is to provide a visually pleasing scar as opposed to a grotesque mass of tissue.
Many case studies now focus on the aesthetic nature of the actual healing process of a wound rather than the probability of infection. This is because generally speaking the rate of infection is low regardless of the technique used.
Although the basic techniques and principles related to tissue repair haven’t changed much in the last century, various options are available to make the overall operation a therapeutic experience.
With the extensive study done in this field, medical practitioners have now developed topical anesthetics, tissue adhesives, and fast absorbing suturing material highly responsible for ensuring little to no amount of trauma for the patient.
The use of sedation during the procedure, especially for difficult cuts, or for an anxious patient, has made suturing easy to tolerate for the family, the physician, and the patient.
A Well-Equipped Suturing Kit is important for optimal suturing. It’s paramount to have the best quality instruments, which are the exact size for the location and nature of the wound that is being closed. The risk of infection is further decreased if the wound is handled carefully, and the instruments sterilized in the correct manner.
It’s very important to consider the suturing material that is used when performing the operation. In turn, choosing the right suturing material is made easy by considering the location and tension of the wound. Other equally important factors to consider about are the tensile and knot strength, handling of the wound, and tissue reactivity.
Suture materials are generally of the following two types:
Absorbable – This type of material is generally used for buried sutures that don’t require removal. They lose their tensile strength in less than 2 months and thus are highly absorbable.
Non-absorbable – This type of material maintains the majority of tensile strength even after 2 months. It is non-absorbable and therefore used to close wounds on the skin’s surface and requires removal.
The needles used for suturing are made exclusively for such a purpose, and comes in a variety of shapes and sizes for a specific wound. Curved needles for example, are only used on dermatological surgery.
Needles are divided into two basic types:
Cutting Needles – As their name suggests, these triangular cross-sectioned needles cut away at the tissue they are placed against. Less force is therefore required to pass the needle but it can leave small puncture wounds in place. They are generally preferred forsuturing of the skin’s surface.
Non-cutting Needles – These are more rounded in the cross section, and are used to push tissue aside and to close it around the suture. More force is used to operate as compared to cutting needles, and is therefore used for organ repair and subcutaneous closure.
Suturing Course and Kit course from The Apprentice Doctor!
There is no need to wait on getting practice with suturing. Before you step into any situation requiring suturing, even an emergency in your own home, you can perfect your suturing skills. The Apprentice Doctor® Deluxe Suture Kit & Online Training Course teaches you how to confidently close wounds. Begin training today!
I really want to become a Doctor – Is there anything I can do straight away?
We often lose sight of the bigger picture while clamoring to pursue our goals. It’s not easy to become a doctor in America, and often factors such as perseverance, expense, family, and time have to be considered before making such a life changing decision.
For some people, the decision to walk this path is a very easy one and goes straight from high school, through college and finally into medical school, never once considering other professions. For others though, the decision is a little bit difficult for it requires an unbiased look at the profession in general, and an objective look at the personality and abilities they possess.
Am I Too Old For Medical School?
For years, nearly all students to be accepted into medical schools were generally 22 or 23 years old, and fresh out of college. Non-traditional students were rarely accepted unless proven to hold an outstanding academic record, and years of research or a similar experience.
This trend has changed now, since more and more applicants for medical schools are older students who had decided to pursue medicine, even after having a different career or any other reason. While, older students often ask of themselves before setting down on his road, it is common to find medical students coming from all ages and backgrounds.
It takes a lot of time and years of study to become a doctor. In addition to the necessary four years of undergraduate study, it takes another four years of medical school then 3-8 years of a residency or fellowship. While it is possible to begin in your 30s or 40s, but anytime after that is not even heard of.
The reason for this is, to get through medical school requires a certain amount of intelligence, and although good study habits and organizational skills are just as important and can make a huge difference in tipping the scales between a mediocre student and a brilliant one.
Academically speaking, the steps of becoming a doctor in America are the following:
Get at least a high school diploma.
Finish a 4 year pre-med program in college/university.
Give a MCAT test in the final year of college/university.
Apply to medical school of your choice, or according to the scores in the test.
The American Medical Application Service is a centralized and non-profit processing service application, for those who need help with finding the best possible medical schools in the country.
Ensuring a good medical school education is one of the most competitive demands that are faced today, just as there is immense competition in the profession itself. It’s quite a challenging task to provide the necessary resources, qualifications, and degree to attendees so that they are able to practice medicine.
As a general rule, wounds are either closed secondarily or primarily. Primary wound closure is one that is operated upon the wound within a short time of its occurrence. The suturing takes little cleaning and preparation which is probably why this type is more popular when it comes to wound suturing. Secondary wound closure is one that is used to suture the wound which hasn’t been closed properly, or there has been a delay in its closure for up to a couple of days since the occurrence of the wound. This is a more complicated procedure to carry out as these wounds have to be meticulously cleaned first. Primary or secondary; which to choose and when
Wounds that are 6 to 14 hours old can be closed using the primary method but only if the wound is not infected. If it is, the wound must be cleaned and treated to remove any traces of an infection before any suturing is performed. On the other hand, wounds that are at 14 hours old or more shouldn’t be closed primarily. Do not use the primary method if any of the following conditions are present:
Reddening around the wound is spreading.
Discharge of pus from the wound.
A constant high temperature.
A mass of soft gaping tissue.
Clearing the wound requires 3 to 7 days of aseptic care along with warm dressings and irrigations. Only then, should secondary wound closure be attempted.
The most important part of a good suturing technique is whether the knot tying method of the suture is correct or not. Different types of knots are used for different types of wounds. Square Knot – One-Hand Technique: A two-hand technique is often used to tie the square knot; however on some occasions it’s not the right technique. In those moments the one-hand square knot technique is used, either the left hand or the right. Square Knot – Two-Hand Technique: This technique used for closing wounds is the considered the easiest and most reliable when it comes to using most suture materials for tying. The same technique can be used with surgical gut, surgical cotton, virgin silk, and surgical stainless steel. Deep tie knot: Tying up a suture in a deep body cavity can be difficult and requires a more complex type of knot. In order to stay tied up, the square knot must be firmly snuggled down. However the operator must perform the suture in a way that avoids upward tension of the suture or else the delicate tissue might tear. Instrument tie: This knot tying technique is particularly useful if/when the ends of both the suture material are short. To get the best results, proceed with caution when using the needle holder, especially when the suture is of a synthetic absorbable type or any other monofilament suture since repeated bending can cause the sutures to break.
Suturing Course and Kit course from The Apprentice Doctor!
There is no need to wait on getting practice with suturing. Before you step into any situation requiring suturing, even an emergency in your own home, you can perfect your suturing skills. The Apprentice Doctor® Suture Kit & Suturing Training Course teaches you how to confidently close wounds. Begin training today!
What do you think? Leave us a comment below.
I really want to become a Doctor – Is there anything I can do straight away?
Medical treatments aim at saving lives and improving health and prevent the spread of infections associated with healthcare provision. Safe injection practices and proper infection control protect patients and healthcare workers. Unsafe injection practices are recognized as a main source of infection in transmitting blood-borne diseases like Hepatitis B, D and C, and HIV. This spurs on the need for safety syringes.
How retractable needles work
The safety or retractable syringe action is similar to a traditional needle except in one aspect. Once you inject the required amount of fluid, the needle retracts protecting from accidental injuries due to needle sticks. Similarly, when you draw blood, you cover the exposed needle with a safety barrel to protect the user from injury.
Need for safety needles
An estimated 5.6 million U.S healthcare workers have a risk of exposure to blood-borne diseases through needlestick injuries and other sharp object injuries.
Healthcare personnel in a hospital setup sustain the number of injuries due to needle stick numbers over 385,000. Nearly 40% of the injuries occur after use and before the sharp devices are disposed of. 41% of the injuries occur while sharp devices are used and 15% of injuries during disposal or after it.
The testing and consequent follow up costs after needle stick injury can go up to $5,000 based on the type of treatment provided.
There is the emotional risk of anxiety and fear faced by healthcare personnel about the consequences like drug toxicity, loss of work time and social implication.
American Hospital Association maintains that a single case of serious infection due to lack of safety needle use can add up to $1 million and more costs related to tests, follow-up, disability payment and lost time.
Saving expenditure
Every product that is introduced to the market at present is more expensive than the conventional or existing products used. This is also the situation in case of safety needles. However, when the product use becomes prevalent and machine cost compensation occurs, the price naturally comes down. Manufacturers generally charge more for safety products, when compared to traditional models and attribute the expense to cost of startup, low volume production, and more parts but this tends to decline with an increase in demand.
Usability of safety needles
While safety needles help in preventing infection and costs, you should account for the convenience and practicality of its use. Convenience is an important criterion. In a survey conducted on the available safety syringe models, the NMT type of safety syringes retracts automatically into the syringe after you empty the chamber, rates at 7.10 on a scale of 10. Single-handed application of the safety mechanism was easy to activate in all models of safety syringes, factors like operation time, accuracy, and prompt use design were favorable, and health care workers preferred the new devices when compared to conventional devices.
Now hospitals are waking up to the advantages present in retractable safety needles and over 20 states in the US have laws and regulations for use of safety devices. While it is important to protect patients, the health care workers should also get adequate protection. The safety syringes bring down the incidences of iatrogenic infection and give cost savings to.
What do you think? Leave us a comment below.
I really want to become a Doctor – Is there anything I can do straight away?
In wound suturing, once the type of needle is selected in performing a surgical procedure, the type of suturing needles is most important. The factors that are considered for the selection of the needle are the size and the purpose, such as sifting through tissue or mending it straight away.
For example, tapered needles are generally used inside the body. Bowels, muscles, or fascia places contain tissue that’s easily accessible and therefore pierced just as easily. Cutting needles, on the other hand, are used for very rough tissue ligaments and skin.
As already noted, the appropriate size of the surgical needle is very important. There are many different sizes and sub-types of needles that are more commonly used for performing wound suturing, and other surgical procedures.
Tapered Suturing Needles
Tapered suturing needles are also called round bodied needles due to their shape and blunt point. Each one is tapered and doesn’t have a cutting edge; therefore, they are generally used for closing soft tissue such as gastrointestinal, vascular, fascia, and other soft tissue found below the skin’s surface.
This type of needle is specially designed for separating tissue fibers rather than cutting them. After inserting the needle, the tissue closes tightly around the suture material, which in turn forms a sort of leak-proof barrier which prevents outside contaminants from entering the wound.
Different wire diameters are used in every round-bodied needle that is manufactured. Each is made according to the type of tissue and wound to be sutured. For example, fine wire diameters are used to repair bowel tissues, whereas a heavier wire diameter is used for suturing muscle.
TP (trigger point): Used to close fascia during abdominal surgery.
CT (circle taper): Used to close the joint space or deep layers of tissue after general surgery.
CT2 (smaller than CT): Often used on closing of uterus.
SH (small half circle): Used to close bowel or tissue layers after breast surgery.
CV: Used for nerve repair and delicate vessels.
Cutting Suturing Needles
These types of suturing needles are used for general closure of skin, subcutaneous tissue, etc, and are sometimes used for ophthalmic and plastic surgery. The point of the needle is triangular and contains a cutting edge. Other than the conventional cutting needle, most surgeons prefer its sub-type, the reverse cutting needle, except when working with tough tissue. The difference between the two is the cutting edge. The edge of a conventional needle is on the inner curvature. The edge of a reverse cutting needle is located on the outer curvature.
Cutting suturing needle types are:
FSLX (for skin/FS extra large): Used for large skin closure, when a lot of tension is present.
FSL (for skin large): Used for the procedures that need a higher tension closure.
FS2 (smaller than FS1): Used for common closing of skin.
P3: Used for closing of small incisions, such as in facial reconstructive surgery and hand surgery.
Learn suturing techniques as part of your medical education, or even personal preparation should you run across an emergency and get to medical personnel. You can use The Apprentice Doctor’s Deluxe Suture Kit & Online Training Course in the privacy of your own home. Practice using high quality suturing instruments on a silicone suture skin model. It’s the ideal kit for student doctors, nurses, and survivalists and preppers.
I really want to become a Doctor – Is there anything I can do straight away?
More commonly known as stitches, a surgical suture is a device used to knit back together body tissues after a surgery done on a person, or because of an injury. The device that is used to do this procedure consists of a needle, and an appropriate length of thread attached to it.
The Attachments of a Suturing Device
The most important attachments of a suturing device are the needle and thread. Over the years, a number of different materials, both natural and artificial, have been used to make the threads. Similarly, the needles used primarily for suturing purposes have evolved from a number of different shapes and sizes to what we are used to today.
Eyed needles – These needles can be re-used. The eyes of the needle are supplied separately from their suture thread, and must be prepared on site for operations. Any thread and needle combination can be attempted with good results with this needle.
Atraumatic needles – Or swaged sutures that come with a pre-packed eyeless needle that is attached to a specific length of thread. This suturing device comprises of an eyeless atraumatic needle swaged or molded by the manufacturer, and comes pre-packaged with a specific length of thread.
The advantage of this type of suturing needle is that unnecessary time is not needed to thread the suture material on the needle.
There are various other types and sizes of surgical needles with which different wound cuts are operated and closed. They include:
Straight edged needle
Compound curve needle
Half curved at both ends of a straight segment (also known as a canoe needle)
Half curved or ski needle
Spiral needles
The Techniques Used For Suturing
Suturing is a method by which wounds that are related to injury or surgery done on a person are closed, and the technique used to do this is nearly 1000 years old.
The only change came with the materials used for suturing and the different aspects of the technique; however, the primary reason for performing such an operation has remained the same and that is:
To close dead space
To give support and strength to the wound, until natural process of healing kicks in
To present the wound for an aesthetical and a functional end result
To minimize the risk of bleeding and infection
Factors Contributing To Aesthetic Wound Suturing
Gentle handling of the scarred tissue is very important for increasing healing capability of the wound. The post-operation appearance of the wound should consist of a flawlessly designed flap, with crossed and zigzagged sutures over the wound, placed with a meticulous and steady hand.
However, if the incorrect suture technique is used to close the wound, or the execution is poor the end result will come out to be grossly disfigured.
Suturing is commonly used today as a means by which wounds are closed in order to prevent infection and hasten healing. Stitches are used by surgeons, doctors, nurses, podiatrists, dentists, first aid workers, veterinarians and survivalists. However, where did the concept for suturing wounds begin?
Archeologists have discovered primitive needles of bone and later metal that were thought to be used for surgical suturing thousands of years ago. It is suggested that the original versions of suture threads were coarse and made from plant fibers before progressing to animal parts much later in history. The first obvious proof of using sutures surgically comes from the Egyptians who used the technique extensively for burial preparation of their mummies. It is assumed that they also used their suturing skills on living people as well. The Greek physician Hippocrates recorded his use of sutures and plant-based materials, but the crude methods and materials most assuredly led to infections and severe scarring during that time of use.
Although the exact date of the transition from plant fibers to animal suturing materials is unknown, the first recorded use of catgut as a suturing material is attributed to Galen of Pergamon in the second century AD. Catgut was and still is made from cattle and sheep intestines, although synthetic catgut is more commonly used today, but like its predecessor, does not require removal because it dissolves in the body.
One of the main problems with suturing surgical incisions and wounds early on was that sterile instruments were not used which often led to skin irritations and infections. In 1860, Joseph Lister addressed the problem by creating a method of for sterilizing suture material by using carbolic acid. Chromic acid was later used to achieve sterilization and then iodine was introduced to sterilize catgut in 1902. These substances greatly decreased the incidents of infection in sutured wounds.
Sterilized catgut has been successfully used for decades and is still in use today. Eventually, however, doctors began to seek other suture options because catgut dissolved unpredictably in different patients which sometimes led to wounds reopening. Scarring was also a major problem with catgut sutures. Synthetic suture materials were produced in the 1920’s and the 1930s saw the creation of two types of surgical sutures, absorbable and non-absorbable which offered doctors a broader choice in suturing materials.
Today, most suture kits contain suture thread made from polymer fiber materials which work well for a variety of surgical suturing procedures. Polymer fiber suture thread comes in a wide selection of styles, designs and types which can be utilized for various wounds and under numerous conditions. Due to its flexible nature, polymer fiber is the preferred choice of physicians, nurses, dentists, veterinarians and first responders and is the best selection for survivalists, adventurers, sports teams and high-risk job workers. Suturing has come a long way since its conception and suture kits offered today contain top sterile equipment and materials to perform wound stitching properly which significantly reduces both infection and scarring.
IMPORTANT! A major website update has been made. Any issues, notify us instantly by pressing the "Quick Help" button and leaving a short description of what you experienced.





















 Learn suturing techniques as part of your medical education, or even personal preparation should you run across an emergency and get to medical personnel. You can use The Apprentice Doctor’s
Learn suturing techniques as part of your medical education, or even personal preparation should you run across an emergency and get to medical personnel. You can use The Apprentice Doctor’s