Suture kits were designed and made for students as a way to help them learn suturing techniques. By practicing on a kit like this, students can improve their skills and techniques before working on real patients. The suture kit includes everything you need to get started and comes with a course that will help you get the most out of your practice suture kit.
The suture kit is the perfect tool for medical professional students like, medical students, dental students, nurses, veterinary students, EMTs, and Emergency Response Personnel. It includes everything you need to practice suturing techniques, comes with a course to help you get the most out of your practice suture kit, and makes it easier than ever to learn how to suture properly.
Problems That Students Have Before Purchasing the Suture Kit and Online Course
Students have a variety of problems before buying a suturing practice kit. These include the following:
Learning the relevant surgical knot tying techniques
Learning suturing techniques
Getting started with suturing
Finding the right suture kit
Ways The Suture Kit And Course Helps Students
The suture kit is a great way for students to practice their suturing skills. The kit includes a variety of suture types, so students can practice their suturing skills on a unique and professionally designed simulation skin pad.
Online courses are also a great way for students to learn suturing techniques. These certified courses offer step-by-step instructions, as well as video tutorials, so students can learn the techniques properly. Students can work at their own pace and at the end of the course they will have to pass a theoretical and practical assessment.
The combination of the suture kit and online courses helps students to become proficient in suturing skills. The kit allows them to practice their skills, while the courses teach them the proper technique.
Get More Out Of Your Suture Kit With These Tips
Suture kits can be extremely helpful when it comes to practicing suturing techniques. However, there are a few ways to get even more out of your suture kit. Here are a few tips:
Make sure you have a good quality kit. There are many different suture kits on the market, and not all of them are created equal. Make sure you select a kit that is made from high-quality materials and that has been tested for accuracy and reliability. The instruments must be of a high professional grade quality and all items (skin pads and suture material) must be available for reorder at a reasonable price.
Practice your suturing skills regularly. It’s important to use your suture kit on a regular basis if you want to improve your skills. Try suturing different types of tissue and using different suture techniques. This will help you become more proficient with the kit.
Ensure that the suture kit that you choose is associated with a certified suturing course.. The Future Doctors Academy Surgical Knot Tying and Suturing Course will take your suturing skills to the next level, by teaching you how to suture correctly. These courses can be found online, while we also offer virtual and in person suturing workshops. The suturing course will teach you everything you need to know about suturing effectively.
Does your suture kit come available in a dedicated kit for right and left handed persons? The Apprentice Doctor Suture Kits do.
The suture kit just got even better!
Here’s What’s New With Our Deluxe Suture Kit:
The suture kit solves a variety of problems for medical students, dental students, nurses, veterinary students, EMTs, and Emergency Response Personnel. It helps them learn suturing techniques faster and more effectively, and makes it easier than ever to get started with suturing.
The suture kit now includes a course to help you get the most out of your practice suture kit.
The suture kit is now easier than ever to use, making it perfect for medical students, dental students, nurses, veterinary students, EMTs, and Emergency Response Personnel.
We also have bi-yearly virtual events you can attend and practice live, online, with other students from the comfort of your home.
The Apprentice Doctor® Deluxe Suture Kit has two types of simulation skin. The 3-layered skin will allow you to practice flap surgery and Z-plasties for instance!
We would love to hear your feedback on improving the suture Kit and Course
The suture kit is ideal for medical students, dental students, nurses, veterinary students, EMTs, emergency response personnel, and even for survivalists. The suture kit includes sutures, suture needles, forceps, scissors, hemostats, and a carrying case – absolutely all the instruments and items that you will need to learn surgical knot tying and suturing. The suture kit is for use in the classroom or on the go. The suture kit is easy to use and comes with a course that teaches you how to suture.
If you are a medical student, dental student, nurse, veterinary student, EMT, or emergency response personnel, you need a suture kit. The Apprentice Doctor suture kit comes with everything you need to suture: sutures, suture needles, forceps, scissors, hemostats, and a carrying case. The suture kit is for use in the classroom or on the go. The suture kit is easy to use and the associated suturing course teaches you how to suture wounds – step-by-step. This course compiled by an experienced surgeon – comes as an absolutely free value add to the suture kit.
I really want to become a Doctor – Is there anything I can do straight away?
Is there a difference between an ER doctor and a trauma surgeon? Yes, there is. When becoming a trauma surgeon, you enter a highly specialized field, interacting with patients facing life-threatening injuries. This article reveals:
The unique skill sets of a trauma surgeon.
A brief history of trauma surgery.
The education necessary to become a trauma surgeon.
Some career options and advancement opportunities for this surgical specialty.
The other day a billboard for a local emergency room went up in my neighborhood. It has a Waiting Time clock on it. That’s a puzzling concept because if you ever need to go to an emergency room, it may not be when the waiting time is only a few minutes.
Most people feel as if their wait time in an ER is hours. That’s probably because an allied health professional has assessed your ailment and determined it isn’t life-threatening. If it is, you’ll be seen immediately and possibly encounter a trauma surgeon.
Both a trauma surgeon and an ER doctor are vital to the controlled chaos associated with the environment of an emergency room. And both respond to emergencies at hand. But since their skill sets are different, their roles are distinct.
A Trauma Surgeon’s Unique Skill Sets
An ER doctor will treat any patient who enters the emergency room, regardless of their presenting condition. One of their primary skills is to stabilize individuals while making decisions about next steps in their care. The majority of patients who have experienced minor trauma, such as cuts and bruises from a fall will see an ER doctor. Once you’ve been released, or even admitted, you’ll usually be assigned to another doctor and not see the ER physician again.
On the other hand, if you fall into a specific medical category, a trauma surgeonenters the scene. Events necessitating a trauma surgeon can range from a serious car accident to a gunshot wound. They are life-threatening because those injuries could affect internal organs. Immediate treatment is necessary by a doctor specially trained to rapidly assess and make decisions about what to do. Trauma surgeons must have confidence in their decisions since often they work with incomplete information.
Although both trauma surgeons and ER doctors must treat patients with compassion and empathy, a trauma surgeon deals with high levels of emotion as well severe physical injuries.
For example, people in terrible car accidents are frequently panic-stricken and confused. Often they go into shock and could be unable to identify everything that’s wrong with them. It’s possible they may not be able to communicate at all. Depression can enter the emotional mix if they feel responsible for the accident, especially if other people were hurt. As a trauma surgeon applies medical knowledge and experience, he or she must also deliver a high amount of emotional support, which requires extraordinarysocial skills.
A trauma surgeon must also think linearly. While assessing a patient, the surgeon treats wounds and injuries in a particular order. Bleeding is stopped first. Next, any potential threat of contamination from open wounds is eliminated. Then a decision about surgery has to be made. Is surgery immediately called for, or is the patient stable enough to transport to intensive care for further treatment and observation? The trauma surgeon must treat injuries while simultaneously thinking three or four steps ahead. Saving a life and preventing permanent damage are the primary objectives. A misstep could be costly.
Common surgeries performed by trauma surgeons include:
Colon
Pancreas
Spleen
Stomach
The Beginnings of Trauma Surgery
The first trauma surgeon in the United States was Dr. George E. Goodfellow, although he didn’t start out with that in mind. In November 1880, he opened up a general medical practice in Tombstone, which was, at that time, located in what was known as the Arizona Territory.
On July 13, 1881, a miner suffered a gunshot wound that perforated his small and large intestines as well as his bowel. Dr. Goodfellow suturedsix holes in his organs. The miner survived due to the quick thinking and immediate surgical intervention by Goodfellow.
Throughout the ensuing years, Goodfellow performed trauma surgery on many notorious outlaws as well as Deputy U.S. Marshall Virgil Earp and his brother, Assistant Deputy U.S. Marshall Morgan Earp, who both suffered gunshot wounds at the O.K. Corral in October of 1881.
Through his many emergency surgical experiences, Goodfellow pioneered the use of sterile techniques in treating gunshot wounds. He ultimately became known as a gunfighter’s surgeon and became the leading authority on managing this type of traumatic injury. His method of what is now known as a laparotomy has become the standard of care associated with penetrating injuries to the abdomen.
Steps to Becoming a Trauma Surgeon
There are multiple steps to becoming a trauma surgeon and you’ll spend 12-15 years in school.
Step 1 – Obtain a bachelor’s degree in biology, pre-med or another science-based discipline.
Step 2 – Complete a doctor of medicine (MD) program, which includes two years of clinical practice.
Step 3 – Enter a medical residency program. If you aspire to become a trauma surgeon, secure one in general surgery so you’re exposed to a variety of surgical procedures. Expect the residency to last 4-5 years.
Step 4 – Complete a 1-2 year fellowship program. During this time you’ll focus on trauma surgeries and receive instruction in follow-up care to patients.
Licensing and Certification
Once you have all the necessary education, you must become licensed and certified. A license is required by law. Certification adds value to your degree and license because an independent third-party has assessed, and approved, your skill level.
You want to pass these assessments the first time you face them. So take the time to study and take practice tests. All the practice you had in medical school allows you to have automatic responses in an emergency. Test practicing gives you the same advantage when answering questions and can reduce any anxiety you may have.
Step 1 – Take theU.S. Medical Licensing Examination(USMLE). This assessment helps state licensing boards evaluate your skills and knowledge. Check with your state for further details.
Step 2 – Although voluntary, you can become certified in General Surgery which requires five years of surgical training before certification is granted by the American Board of Surgery.
Step 3 – Once you receive your certification in general surgery, you can also obtain a subspecialty certification from the American Board of Surgery. They offer five subspecialty certificates, but the best one for trauma surgeons is the Surgical Critical Care certificate. A surgeon specifically trained in this area has skills in diagnosing and treating trauma victims with severe infections and organ injuries.
Acute Care Surgery
The American Association for the Surgery of Trauma defines Acute Care Surgery (ACS) as a developing area of medicine consisting of three components – trauma, critical care and emergency surgery. The need for trauma and emergency surgical care has increased over time, requiring improved, formal education covering both areas. As a result, the Trauma and Acute Care Surgical specialty emerged. Your formal trauma education may incorporate this ever-growing concentration.
Continuing Education
In the field of medicine, continuing education is mandatory. Trauma surgeons must stay abreast of advancements in surgical techniques. The better the methods and tools, the less risk there is to patients. Educational content varies depending on a doctor’s specialty. However, the surgical material is more complicated. Minimal requirements for continuing education are ten hours of participation in an accredited continuing medical education program. TheAmerican Medical Association(AMA) is a source of information for CEUs.
Career Advancement
Trauma surgeons are nearly at the top of their field. However, depending on your years of experience and the competency of your skills, you may be asked to participate in research and development. R&D tends to focus on the advancement of surgical procedures and techniques. You may also elect to mentor and teach medical residents just starting out on their career path.
Career Options for Trauma Surgeons
Although you may consider a hospital as the only place that employs trauma surgeons, there is a vital need for them elsewhere. Becoming a member of the military or naval medical staff, are career options. Unfortunately, injuries to soldiers are often traumatic, and skilled surgeons capable of remaining calm and effectively performing in high-stress situations are always needed.
Entering the field of medicine can be a gratifying career. But the role of a trauma surgeon is one where your intervention means the difference between the life, and death, of an individual.
Can you begin your career in trauma surgery today?
Indeed yes!
The Apprentice Doctor® Academy has developed and perfected an Online Course for Future Doctors to assist them towards fulfilling their dreams of becoming great medical professionals. TheFor Future Doctors Foundation Medical Online Course with accompanying Medical Kithas helped launch the career of thousands of want-to-be doctors!
The Apprentice Doctor® Suturing Course and Kitis a resource that will teach you how to suture wounds in a couple of hours! If you want to become a Surgeon – why not learn how to suture wounds now?
If you’re interested in medical school and becoming a doctor or surgeon, these articles may be of interest to you:
The blending of surgery and engineering isn’t unheard of, although rare. But it’s clear that engineers and surgeons are working together to make miraculous progress in the field of medicine. These advances are making surgeries shorter with less risk to patients.
This article gives you a snapshot of a few engineering advances making positive changes in surgical procedures:
If you are interested in becoming a medical engineer, you’ll also find information on that fast-growing career.
Becoming asurgeonand an engineer so that they blend into a single career is an interesting proposition. The advantages seem clear, but the concept isn’t straightforward. Being a surgeon can enhance medical engineering research and surgical advances. The critical thinking and problem solving skills of an engineer are similar to those needed by a surgeon. Although years of education are required to secure both degrees, the knowledge of one can complement the knowledge of the other. I’m aware of one doctor who holds a degree in electrical engineering as well as in otolaryngology, neurological surgery and urologic surgery.
If you have ever considered a dual title such as medical-surgical engineering, you’ll have to know as much about medicine and medical practice as you will about electronics, biomedical technology and chemical engineering.
When surgeons and engineers work cooperatively, yet independently, here is a snapshot of what they’ve been able to accomplish.
Types of Engineering Technology Used in Surgery
Stretchable Electronics
What they are: Although stretchable electronics can be used in a variety of industries, in the medical industry they perform like adhesive bandages. They can bend, stretch and otherwise mold themselves around multiple surfaces. The sensors embedded in them can send data from the human body back to the surgeon or other healthcare professional.
The initial challenge: To develop “stretchy electronics” so a single surgical instrument could be used in open heart surgery instead of three, reducing the risk to the patient. During open-heart surgery, surgeons often have to utilize multiple balloon catheters with different functions. Because they all have to be inserted sequentially, surgeries are long, complicated and sometimes painful. The longer the surgery, the higher the risk to the patient. Currently three different devices have to be used. The first maps the heart’s signals so the problem area can be identified. The second one controls the positions of therapeutic actuators and their contact with the epicardium. The third is used to burn away damaged tissue.
The initial solution: Development of a multifunctional balloon catheter that stretches up to 300%, inflating or deflating as needed in the surgical procedure. It operates reliably without any changes in properties.
Advantages/Applications:
Delivery of high-quality information such as temperature and blood flow to surgeons in real time.
Neuroscience research.
Performs corrections on heart tissue during surgery through the use of radio signals to heat and kill cells.
Physical rehabilitation.
Preemie monitoring.
Provides fast, high-resolution mapping.
Quickly diagnoses and treats the causes of irregular heartbeats.
Spinal surgery.
Sun exposure monitoring
Future Adaptations:
Biodegradable implants to monitor cranial pressure and temperature.
Collection of bodily fluids to monitor electrolytes and glucose levels.
Monitor the risk of asthma attacks in the lungs.
Monitor the stretch and flow of bladder functions.
Real-time mapping of electrical activity in the brain during epileptic seizures.
Electronic Surgical Gloves and Finger Sleeves
Image: John Rogers/University of Illinois
What they are: Similar to stretchable electronics, semiconductors embedded in soft, flexible surgical gloves allow cardiac surgeons to feel everything they do with their fingertips.
The initial challenge: Reduce the size of current technology, which is large and bulky. There was a need for a simple technology that could measure the stress and strains during surgery through the fingertip(s). With electrotactile simulation surgeons could monitor and detect medical information from the skin.
The initial solution: Integration of ultra-thin and stretchable silicon-based electronics and sensors with artificial skin that can be slipped on hands or fingertips.
Advantages/Applications:
Performs ultrasound imaging of tissue upon touch.
Performs surgery by heat-induced local ablation.
Precisely removes tissue using local ablation.
Relays information such as temperature, conductivity, etc. to the skin.
Senses the electrical properties of tissue.
Future Adaptations:
Application of sensors to flexible surfaces to provide a sense of touch to prosthetic limbs.
Measuring motion and temperature.
Softer robotic interactions with surroundings.
Wrapping the surface of the heart with sensors to diagnose and treat cardiac arrhythmia.
Needlescopic Surgery
What it is: Minimally invasive, needlescopic surgery uses instruments with a diameter 10,000 times thinner than a strand of hair. The incisions can be sealed with surgical tape. Scars are small if they exist at all.
The initial challenge: Reduce the invasiveness of surgeries through the use ofneedle-sized instrumentsthat current robotic technologies can’t accomplish.
The initial solution: Provide needlescopic surgical instruments that possess more dexterity, thereby broadening potential applications.
Advantages/Applications:
Laparoscopic surgery.
Less postoperative pain.
Minimally invasive surgeries in small areas such as the ears, nose and throat.
Shorter hospital stays.
Transnasal brain surgery.
Future adaptations:
Currently very few surgeons in the world use needlescopic surgery. As more surgeons incorporate it into their practices, future adaptations can be better identified.
Robotic Surgery
What it is: Robotic surgery is another type of minimally invasive surgery. Through the use of miniaturized surgical instruments mounted on one of four robotic arms, it allows surgeons a maximum range of motion and precision.
The initial challenge: Provide surgeons a way to perform complex procedures with more precision, flexibility and control than is possible with conventional techniques.
The initial solution: The creation of a robotic surgical system controlled bysurgeonsat a computer console near the operating table. The two most well-known systems are the da Vinci and Zeus.
Advantages/Applications:
Robotic surgical system on a test medical stand
Clearer visual field.
Fewer complications, such as surgical site infection.
Greater flexibility and precision during surgery.
Increased mobility without tremors.
Less pain and blood loss.
Perform surgeries previously too high risk with current techniques.
Quicker recovery.
Smaller incisions and scarring.
Future Adaptations:
Expanded opportunities for teaching and assessment of new surgeons.
Integration of new and current technologies used in surgical procedures.
Long-distance intraoperative consultation or guidance.
Preoperative and intraoperative video image fusion to better guide surgeons in dissection and identifying pathology.
Rehearsal of complex procedures before performing them on patients.
Medical Engineers
Blending engineering and surgery into one role is possible, but takes many, many years of schooling. As an alternative, if you want to work in medicine with an engineering degree, you may be interested in becoming a Medical Engineer.
Medical engineers apply engineering principles from technical sources to solve clinical problems. As you have read in this article, they have created medical products that combine anatomy and physiology with technology. The result is higher quality healthcare for surgical patients. Future research shows similar advances in all areas of medicine.
As a medical engineer, you can go in any number of directions. Research, development and quality assurance represent only three areas. The development and evaluation of medical devices is another. You can help hospitals and medical clinics with the latest purchases in biomedical technology by evaluating their needs against what’s available. You can also specialize in nanotechnology, stem cell research, or other areas of cutting-edge medicine. The avenues that combine healthcare with electronics are expanding all the time.
To be successful in the field of medical engineering, you must be able to give attention to detail, creatively solve problems, and apply analytical thinking. Because you’ll be working with others, you must be able to easily integrate yourself into a team by expressing ideas and listening to others. More often than not you will have to be a leader.
To enter this field you must obtain a bachelor’s degree in engineering, physics or related program. You will need to go on to graduate with a master’s or Ph.D. in medical engineering.
Would you like to start learning surgical skills today? You can!
Would you like to develop the skills used by a surgeon or medical engineer? There’s no need to wait until you get into a post-secondary or graduate program. You can begin right now.
The Apprentice Doctor® Academy has developed and perfected an Online Course for Future Doctors to assist them towards fulfilling their dreams of becoming great medical professionals. TheFor Future Doctors Foundation Medical Online Course with accompanying Medical Kithas helped launch the career of thousands of want-to-be doctors!
The Apprentice Doctor® Phlebotomy Course and Kitis a resource that will teach you how to confidently perform phlebotomy procedures in a couple of hours! If you want to perfect that skill, why not learn how to perform venipuncture procedures now?
The Apprentice Doctor® Suturing Course and Kitis a resource that will teach you how to suture wounds in a couple of hours! If you think may be drawn to direct-patient care, why not perfect suturing techniques now?
If you’d like information about becoming a surgeon, you may be interested in the following articles:
Provide indirect patient care and still be a vital member of a medical team
Story at a Glance
Many people in healthcare work behind the scenes. They like the idea of helping people, and want to work in the medical field. But they prefer work environments that are calm and quiet. A medical lab technician job may be just what you’re looking for. This article covers:
6 common characteristics signaling a healthcare technician job may be right for you.
8 indirect patient care careers.
Medical/Clinical Lab Technician
Cytogenetic Technician
Histotechnician
Pathology Assistant
Nuclear Medicine Technician
Anesthesia Technician
Radiation Protection Technician
Medical Equipment Repair Technician
The education and credentialing required for each.
Are you interested in healthcare, but prefer working behind the scenes? We hear a lot about careers that provide direct patient care. But it may surprise you to learn there are indirect patient care medical careers available. These medical lab technician roles are important in field of medicine and today we’re going to give you a snapshot of eight of them.
Medical/Clinical Laboratory Technician
Cytogenetic Technician
Histotechnician
Pathologist Assistant
Nuclear Medicine Technologist
Anesthesia Technician
Radiation Protection Technician
Medical Equipment Repair Technician
6 characteristics signaling a healthcare technician job may be right for you
Are you a little uncomfortable interacting with people all the time? Feeling drained of energy when talking with others without periods of quiet could mean you’re introverted. That means you need time away from lots of activity in order to recharge yourself. Extroverts, on the other hand, gain vitality from being around people. That’s how they rejuvenate themselves. The good news is that healthcare needs both types of personalities.
Even if you identify yourself as an introvert, you may still wonder if a laboratory-type job is right for you. If any characteristic of the following six sounds like you, it could be.
You enjoy science – The careers we’re reviewing in this article all have a basis in chemistry, biology, and physiology. If you enjoy science, chances are high you’ll be happy in at least one of these careers. Don’t worry if you didn’t like science in school. Interests change over time. All you need are a strong sense of curiosity and enjoyment in learning.
You attend to detail – You’ve probably worked with people who don’t pay attention to details. As a result, mistakes get made, and tasks have to be done again. But if you’re someone who is meticulous and precise in gathering particulars, then medical labs need you. Many of these indirect care careers have to analyze and compile data to help doctors diagnose and treat their patients.
You strive for consistency – If you agree that consistency in work can be reached through repetition and routine, then working in a lab may be perfect for you. If you’re someone who can repeat tasks and remain focused and careful, lab analysis and research positions are good options for you to investigate.
You prefer working with patients indirectly – As you may have guessed by now, you don’t have to be interacting with patients all day to make a difference in their lives. A career in a laboratory medicine allows you to play an integral role in the healthcare system without being center stage. Even if you sometimes have to draw blood, or provide instructions to people about what they need, the majority of your time will be spent in a non-chaotic, secluded work environment.
You desire job security – Allied health technician jobs are relatively secure and stable. According to theBureau of Labor Statistics(BLS), on average, jobs for medical technicians are projected to increase at a faster-than-average rate of 14% through 2026. A contributing factor for the growth is an aging population with ongoing medical issues.
You want to begin your career quickly – Many healthcare careers require an extensive education. Most medical lab technician training programs can be completed in two years or less. That means you’ll be in the field a lot sooner.
If any of these attributes describes you, then you may be someone who is well suited to laboratory and research work in healthcare.
8 medical lab technician careers
Of the following 8 careers, no one is more important than the other. Although some of the duties of each job may be similar, what is studied and researched is not. When sifting through the options, consider what appeals to you most.
Most of the careers fall in the category of Medical/Clinical Lab Technician (MLT), although there is also a job title specifically related to that. We’ll cover the general MLT first, then proceed to specific specialties within the medical lab technician field.
Medical/Clinical Lab Technician
Job Responsibilities: Lab technicians, or MLTs, work with integrated systems and perform mechanical or diagnostic tests in medical laboratories. Some MLTs work independently while others prefer to work in companies where they’re part of more extensive teams of professionals.
Lab technicians perform a variety of tasks. Collecting samples, studying and performing tests on anything from bodily fluids to biopsies are only some of the functions you’ll perform. You’ll use a variety of equipment and software programs to conduct thorough and accurate tests. You’ll also be expected to record information you discover for review by doctors, physicians and scientists. Maintaining and sterilizing your lab equipment are also elements of the job.
From time to time you may be asked to acquire samples from patients, but won’t establish ongoing relationships them.
Lab technicians work in a variety of medical settings. Dental offices, clinics, and ophthalmic labs are only a few.
Education Required: For the most part, to become a technician, you’ll need an associate degree. If you aspire to become a technologist, you’ll have to pursue a bachelor’s degree. Both degree levels include coursework in biological sciences, lab management, chemistry, and statistics. Although there are short-term certificate programs available, you may discover an individual with more education is given preference by employers. Associate degree programs last 18-24 months. Bachelor degree programs require a four-year commitment.
Regardless of the educational path you select, you’ll learn how to use medical laboratory equipment and how to conduct data analysis. You’ll also explore content such as immune hematology and become proficient in studying biological samples.
Some ophthalmic and dental labs may be willing to provide on-the-job training. In those situations, you can get started with only a high school diploma. However, to be hired in a medical or clinical lab, you typically need an associate’s or bachelor’s degree. The higher your level of education, the better your chances are of being hired.
Key Skills: To be a successful MLT, you must be able to:
Communicate accurately and efficiently.
Demonstrate solid analytical skills.
Focus on details.
Manage time effectively.
Operate independently.
Work with a team.
Cytogenetic Technician
Job responsibilities: A cytogenetic technician is a type of MLT who analyzes genetic elements inside cells. As a cytogenetic technician, you’ll analyze chromosomes and other genetic materials. You’ll also maintained detailed notes for each sample. This includes ensuring any sample is associated with the correct patient. Overall you’ll study cells at a microscopic level for signs of irregularities or disease. The work is completed in a medical facility or research institution, where there is a lab manager, and you’re a member of a cytogenetic team.
Education required: Generally, a bachelor’s degree in cytotechnology, biological science, or chemistry field is required. You’ll encounter topics such as cellular biology, biochemistry, and genetics. Most programs contain a clinical aspect where you’ll gain hands-on experience while working under the supervision of a qualified instructor. It is recommended you attend an accredited program. For more information on cytotechnology training programs, you can visit theAmerican Society for Cytotechnology(ASCT).
Credentialing: Following graduation from an accredited program in cytotechnology and gaining experience in the field, candidates for credentialing may qualify to take one of the American Society of Clinical Pathology (ASCP) Board of Registry exams. Some states may require regional testing. Check your state for their criteria.
Key Skills: Successful cytogenetic technicians possess the following skills:
Ability to set up and operate sophisticated laboratory equipment.
Analytical or scientific competencies.
Proficiency in using a database and query software.
Project management.
Histotechnician
Job Responsibilities: Professionals who study the minute structures of biological material and determine how they are structurally and functionally related are called histotechnicians. The field encompasses how biochemistry, molecular biology, and physiology interact with disease processes. Like other MLT specialties, you’ll be studying and analyzing samples and reporting data to researchers, doctors, and scientists.
Education Required: Initial preparation for a histotechnician begins in high school with a strong curriculum in biology, chemistry, math and computer science. The next step is attending an histotechnician associate degree program accredited by theNational Accrediting Agency for Clinical Laboratory Sciences(NAACLS). You may be able to attend a community college, or even a hospital training program. If possible, while you’re going to school, try to work part-time in a lab setting to gain experience. If you want to become a histotechnologist, you will need a bachelor degree.
Credentialing: Although certification is voluntary, many states require you to have a license. TheAmerican Society for Clinical Pathology Board of Certification(BOC) facilitates the exam. Since licensing requirements differ significantly from state to state, you’ll have to check your state for their criteria.
Key skills: Successful histotechnicians must be able to:
Analyze difficult problems.
Communicate effectively.
Gather samples.
Make sound decisions.
Manage time efficiently.
Manipulate small tools.
Meet deadlines.
Understand and perform tissue staining protocols.
Pathologist Assistant
Job responsibilities: First and foremost, a PA helps a pathologist prepare and diagnose tissue, blood and other specimens in a sterile laboratory. Depending upon the work environment, as a PA you might also examine corpses to determine a cause of death. Tasks could include collecting and dissecting postmortem specimens, conducting various tests on samples, taking diagnostic images, and recording your findings. From time-to-time some PAs may be asked to train colleagues or assist with autopsies, which does require some social interaction. However, most responsibilities are lab-based and can be performed independently.
Education required: Federal law requires PAs to have a minimum of an associate degree (American Association of Pathologists’ Assistants). You may choose to complete a bachelor’s or a master’s degree in the field. Most PA programs take about two years to complete. The curriculum consists of science courses like microbiology, genetics, and immunology. Students will also encounter pathology courses. Nearly all programs provide clinical experiences.
Credentialing: PAs may seek a three-year certification through theAmerican Society for Clinical Pathology. Some states require additional criteria and even state licensing before you can begin work. Check your state for details.
Key skills: Successful pathology assistants will demonstrate:
Active listening skills.
Analytical/scientific thinking capabilities.
Attention to detail.
Competency in information ordering (following rules or arranging data/actions in a specific order).
Proficiency in using information systems software.
Nuclear Medicine Technologist
Job responsibilities: A nuclear medicine technologist performs imaging tests that help doctors identify abnormalities inside the body. The process involves giving patients small doses of radioactive materials and then using specialized equipment to record images of organs or other body parts where the substances localize. As a nuclear medicine technologist, you’ll have some interaction with patients when you explain procedures to them. You’ll also inspect equipment and possibly administer the radiopharmeceutial material, which is given orally, by injection, or through inhalation.
There are inherent risks in this job. You may be exposed to infectious diseases as well as to radiation. Consequently, you must take measures to protect yourself and be precise in following those protocols.
Education required: An associate or bachelor’s degree in nuclear medicine technology is necessary to enter this field. If you already have a degree in a related science, you may be able to combine that with a 12-month certificate program and enter the profession a little faster. In addition to courses in anatomy and physiology, you’ll be in classes about nuclear physics and radiochemistry.
Credentialing: Many states require a license to practice. See the Society of Nuclear Medicine and Molecular Imagingto find out if your state is one of them. You can also check with your state health department for current rules and regulations.
Two professional organizations, theNuclear Medicine Technology Certification Board(NMTCB) and theAmerican Registry of Radiologic Technologists(ARRT), offer voluntary certification. Some states that license nuclear medicine technologists will accept this certification. Others will require you to take an exam. Even states where certification isn’t needed, it is advantageous to have certification because it can improve your chances of being hired.
Key skills: Nuclear medicine technologists must possess the following skills:
Ability to work as a member of a team.
Attention to detail in data recording and observations.
Decision-making capabilities.
Strong communication skills.
Technical know-how to operate complicated equipment.
Anesthesia Technician
Job responsibilities: If you enjoy working with machinery, but also being a member of a care team with indirect responsibility for patients, then a career as an anesthesia technician may be right for you.
Professionals in this technical role contribute to safe anesthesia care by providing support to the anesthetist. This may include ensuring the anesthesia equipment is working properly, to assessing dosages of medications given to patients. As an anesthesia technician, you are part of a surgical team and will have some interaction with its members as well as with patients.
Education: A high school diploma is the minimum education required, although anesthesia technician degree programs are available. If you’re a high school student, focus on courses in math, science, and technology. Anesthesia technician degree programs will include curriculum topics like pharmacology and anesthesia equipment functionality. At least one year of experience in the field as an intern is recommended.
Credentialing: Although certification is voluntary, there is a national certification exam available that could increase your potential employment opportunities. The national exam is conducted by theAmerican Society of Anesthesia Technologists and Technicians(ASATT) and is the only one officially recognized. During your job search, ensure you have documentation of a basic life support certification since this is a requirement in any hiring situation.
Key Skills: To be successful as an anesthesia technician, you must:
Be comfortable working with computers, biomedical equipment, and anesthetic devices.
Communicate well.
Focus on details.
Problem solve.
Radiation Protection Technician
Job Responsibilities: Although not specifically a medical lab job, radiation protection technicians provide a valuable service to overall public health. RPTs are also referred to as nuclear monitoring technicians or hazardous materials removal workers. As the titles imply, RPTs track radiation levels. They also expose leaks or potential hazards and then remove them. As an RPT you may even find yourself organizing evacuations of contaminated areas. The type and seriousness of the emergency determine the protocol followed. Some RPTS specialize in decontamination, emergency response or storage, and disposal. Or you’ll analyze environmental samples to determine levels of contamination.
There are risks involved in being an RPT. You may be exposed to contaminated material or radiation. Training programs provide extensive information on how to protect yourself, thereby minimizing your risk factors.
Education Requirements: Because there are specializations within the field of radiation protection, the type of training varies. Many positions require a certificate or associate’s degree in radiation safety or technology. Some employers may provide on-the-job training.
Formal programs are heavily based in math and science. You’ll also learn about radiation safety, contamination control, and radiological chemistry. The structure and nature of nuclear or power plant systems are generally included as part of the curriculum. There’s little doubt you’ll have lab and internship experiences along with the didactic portion of your studies.
Credentialing: TheOccupational Health and Safety Organization(OSHA) is the federal entity that maintains and audits regulations concerning the safe removal of radiation and nuclear waste. As a result, professionals who work with and remove those products must undergo a mandatory 40-hour training course. You may also be required to complete three months of additional training through theNuclear Regulatory Commission(NRC). This additional training provides information about the protective gear you’ll wear, the equipment you’ll use, and the materials you may encounter.
Key Skills: A successful radiation protection technician will demonstrate:
Attention to detail.
Calm demeanor in crisis situations.
Capability to work independently with accuracy and precision.
Communication skills.
Cooperative attitude in working with a team.
Critical and logical thinking.
High energy.
Mechanical aptitude.
Medical and anatomical competencies.
Time management efficiencies.
Medical Equipment Repair Technician
Job responsibilities: Although this technician job may feel non-medical, it is critically important to all medical facilities. When healthcare equipment breaks down, it must be repaired – and repaired quickly. If it doesn’t work correctly, a potentially severe illness or disease could be missed or misdiagnosed. So medical equipment repair technicians are vital members of all medical teams even though the care
provided to patients is indirect.
The duties of a medical equipment repair technician vary by type of equipment, but most repair technicians
install, clean, maintain and fix medical equipment. Within those primary tasks, you’ll keep detailed service records and be presented with the latest updates in equipment software. You may even learn how to use and install the newest equipment available on the market. Although the scope of this profession is outside of a medical laboratory, the work is independent and a few steps removed from excessive chaotic environments.
Education required: Due to the sophistication of medical equipment, it’s best to obtain an associate’s degree in biomedical equipment technology. In this kind of a training program, you’ll learn hardware and software repair, electronics and physics. Because the equipment is designed to inspect the human body, you’ll also learn medical terminology and anatomy and physiology. Throughout a training program you’ll be exposed to a generous variety of medical equipment where you’ll learn to identify and correct mechanical problems. A bachelor’s program offers more in-depth content where you’ll encounter more complex and electronic-based medical equipment.
Credentialing: While registration, licensure, or certification isn’t mandatory, employability may be improved if you obtain certification through the Association for the Advancement of Medical Instrumentation(AAMI). Three types of certification are available. A certified laboratory equipment specialist (CLES), a certified biomedical equipment technician (CBET), and a certified radiology equipment specialist (CRES).
Key Skills: A capable medical equipment repair technician must possess or acquire:
Comfort in working independently with minimal supervision.
Decision making capabilities.
Dexterity.
Mechanical, safety testing, and troubleshooting skills.
Precision in the work environment.
Problem solving competencies.
Stamina.
Strong communication style.
Time management efficiencies.
Conclusion
Each occupation listed provides a calm and quiet work environment. For individuals who gather energy in this type of setting, one of careers may be a perfect fit for you. Although all require small to moderate interactions with patients or colleagues, none of them provide direct patient care. Education requirements for most of them are minimal so that you can get into the field quickly.
Before making any final decision to obtain a certificate or degree, talk to a few people in the field. Find out what they like about their careers, and what some of the drawbacks are. Discussions like these will help you narrow your career choices so that you can make the one best suited to your interests and personality.
Thank you for stopping by today.
Would you like to start learning lab skills today? You can!
Several of the medical lab technician careers outlined in this article require drawing blood. You can practice that skill right away.
The Apprentice Doctor® Phlebotomy Course and Kitis the resource that will teach you how to confidently perform phlebotomy procedures in a couple of hours! If you want to perfect that skill, why not learn how to perform venipuncture procedures now?
You may decide you prefer direct-patient care. If that’s the case, you may be interested in wound suturing.
The Apprentice Doctor® Suturing Course and Kitis a resource that will teach you How to Suture Wounds in a couple of hours! If you think you may be drawn to direct-patient care, why not perfect suturing techniques now?
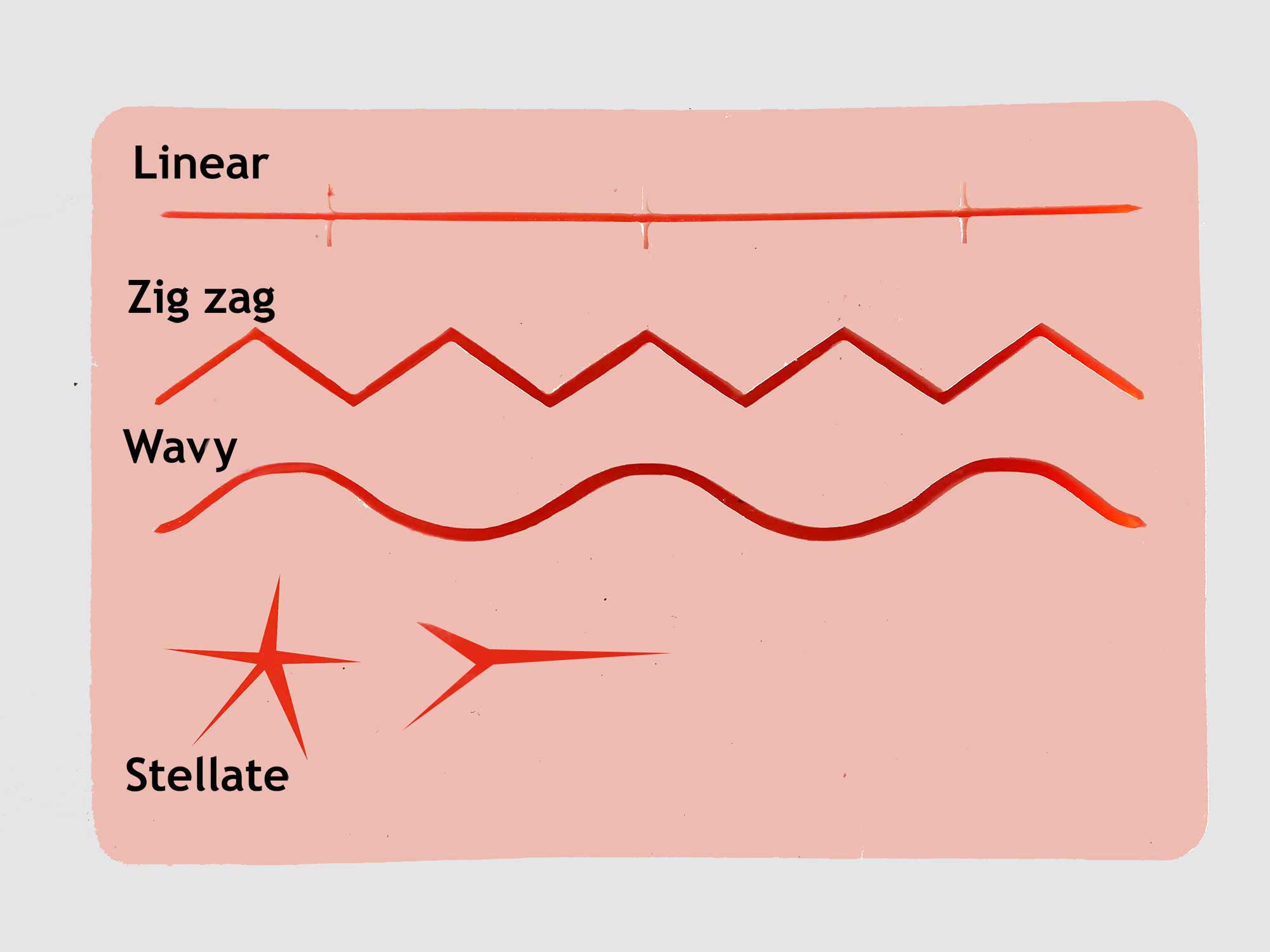
When a surgical wound heals properly, the sutures around its edges stay intact while new tissue, known as “granulation tissue,” starts forming. One of the most common complications of surgical wounds is when the surgical incision breaks along the suture. In other words, the wound splits open, a condition known as wound dehiscence.
Why does wound dehiscence occur?
Wound dehiscence is caused by many things such as age, diabetes, infection, obesity, smoking, and inadequate nutrition. Activities like straining, lifting, laughing, coughing, and sneezing can create increased pressure to wounds, causing them to split. Chronic use of corticosteroids (steroid hormones made in the adrenal cortex or synthetically), previous scarring, the presence of radiation at the incision site, improper stitch usage, unsuitable suture type, fluid-coagulant balance, cancer, and surgical errors can also contribute to wound dehiscence.
Dehiscence can also occur due to poor wound undermining throughout the surgery. Wound undermining means that damaged tissue extends under the skin and can’t be seen on the surface.
The location of the wound can also cause dehiscence. For example, wounds located on the legs, shoulders or back, or in mobile areas or areas prone to high tension, are at increased risk of rupturing.
Patients diagnosed with Ehlers-Danlos syndrome are more likely to experience dehiscence. Ehlers-Danlos syndrome is an inherited disorder that affects connective tissue, particularly skin, joints and blood vessel walls.
Symptoms of wound dehiscence
Some common symptoms of dehiscence are:
Broken sutures that don’t heal.
Bleeding from wound and bleeds at the surgical wound entry points.
Fever.
Inflammation.
Pain at the wound site with high sensitivity to touch.
Sudden opening of the wound.
Swelling.
Wound drainage – pus-filled and frothy.
A frequent effect of wound dehiscence is arterial bleeding. Blood from an arterial bleed is brighter in color and may spurt, or pulsate. Arterial bleeds occur more often in patients who are overweight or suffering from diabetes.
Causes of wound dehiscence
One of the leading causes of wound dehiscence is infection. Some characteristic signs of infection are:
Abscess – swollen area that contains pus.
Erythema – abnormal redness of the skin.
High body temperature.
Large amounts of exudates – seepage from the wound area.
Odor.
Severe pain.
How is wound dehiscence treated?
Dehisced wounds require immediate attention. After the wound is sutured closed, doctors primarily use one of two methods to treat dehiscence.
Antibiotics – Use of an antibiotic ointment over a newly sealed wound may prevent any possible future infections.
Debridement – Removal of any dead or damaged tissue from the surgical wound. Doing so creates a better seal for a new surgical closing. It can also improve the development of healthy skin tissue.
If a wound has previously suffered a dehiscence, it must be monitored closely. Careful observation minimizes any issues that may occur during this second healing process.
13 possible reasons for wound dehiscence
Although there are many reasons that contribute to wound dehiscence, what follows are the most common.
Utilization of inappropriate knot
The importance of proper suture knot techniques
When it comes to suturing, knots are much more than tying off the ends of materials passed through body tissues. Maintaining appropriate tension on the suture is vital to healing, so knots have to be set properly to ensure stitches remain intact.
Surgeons determine what type of knot to use when closing wounds. In the picture below [1], from left to right, are three frequently used:
Simple knot – incomplete basic unit
Square knot – completed common knot
Surgeon’s or friction knot – completing tension
How suture material and suture experience affect knots
The knotting technique used depends mainly on the nature of suturing material. For example, multifilament materials are those that are made by braiding or twisting so that the coefficient of friction rate is high. As a result, knots hold well and remain tied as they are created. Monofilament materials consist of only one strand of fiber, and their coefficient of friction rates are much lower meaning that they tend to come untied more easily. Also, synthetic polymeric monofilament suture materials have “memory” which means they tend to return to their original shape instead of lying flat, which is a desired quality in suturing.
The quality of suture knots is also a product of the skill of the person applying them. The positioning of knots is determined by the suture technique and wound being treated. These decisions determine how secure the knot remains. Using the wrong knots or tying them too hastily compromises knot quality.
Potential problems caused by improper suture knots
Proper suture knots are vital to the overall suturing process to ensure that wounds heal effectively.
Improper suture knotting techniques can cause the knots to loosen or come undone entirely. This, in turn, relieves the holding tension of the suture, allowing the wound to open. An open wound will not heal correctly, causing infection or excessive scarring. Incorrect knotting techniques can also leave too much material remaining which not only becomes a snag hazard but can produce more significant irritation and discomfort to the patient.
Knowing which suturing knot technique is appropriate is essential since the primary focus of wound suturing is to create closure for the wound. When suturing is done correctly, it reduces bacterial entry, heals properly, and produces the least scarring possible.
Tying knots too loosely
If suture knots are applied too loosely, they can allow the suture to slip and lose tension. Loose knots snag easily during daily activities which can cause the stitch to break, increasing the possibility of the wound opening. If a suture is not held under its ideal tension by a correctly tied knot, the healing properties of the wound will be compromised. This can lead to improper healing, and bacteria may enter the wound creating infection, excessive scarring, and greater discomfort.
Sutures and knots can become loose even when they have been applied properly. The objective is to repair the suture before any lasting damage occurs to the wound. Suture tension must be regained to keep the wound closed, allow for full healing, resist infection, and minimize discomfort and scarring.
Employment of improper suture material
Heavier suture materials provide the best tension strength for holding wounds closed, and require fewer and more secure knots. Lighter materials cause less tissue irritation and damage and glide through wounds more efficiently. But they need several knots for adequate closure. Thin suture materials, therefore, are selected for cosmetic areas, such as the face, to produce less scarring. If a thick suture material is used on the face, more noticeable wound and suture track scars are the results.
Also, using absorbable versus non-absorbable or braided versus non-braided suturing materials incorrectly can lead to problems. Absorbable materials dissipate over time and do not require removal. Such materials can be somewhat unpredictable in their breakdown which, if used on surface wounds, can occur early leaving them prone to opening or tearing.
The choice between using braided or non-braided sutures is just as important. Braided materials are woven together and provide better knots and wound tension, but are also considered causes of more adverse skin reaction. Additional, they can present a higher risk for infection due to the presence of grooves where germs can enter the wound.
Selection of the incorrect needle
One of several types of needles can be selected for the suturing process. Two primary ones are cutting needles and round body needles.
Cutting Needles – Cutting needles have two sharpened point edges that oppose one another. This design is for use on dermal tissue that is tough and difficult to penetrate, such as dense, thick and irregular connective tissue. Variations include conventional cutting needles and reverse cutting needles. Traditional cutting needles have a three-blade, triangular-shaped tip that is sharpened on the inner convex for better penetration and a flattened body which is more easily grasped by a needle holder. Reverse cutting needles have sharpened edges on the outer convex and are used to suture extremely tough yet delicate dermal tissue such as oral mucosa and tendon sheath.
Round Body Needles – These suture needles have a tapered, sharpened tip and a round body designed to pierce instead of cut skin tissue. The grasping end is rectangular or oval for better holder control. Round body needles are used in soft, easily penetrable tissue, such as subcutaneous layers, abdominal viscera, peritoneum, myocardium tissue, etc.
Cutting needles cause less injury to tough types of tissue because it will penetrate the tissue with minimal force as opposed round body needles where excessive force is needed to penetrate the tissue – but it may actually cause more damage in softer tissue like fascia – by tearing through the tissue causing damage and scarring. When this happens, it may indirectly increase the risk of infection.
Some bodily structures are quite thin and friable, so always remember a cutting needle can cut through the tissue like a scalpel. Consider using a reverse cutting needle in certain situations.
Over-tightening of sutures
The importance of not suturing wounds under tension is emphasized in most surgical skills and suturing courses. Excessive pressure may cause the suture to break and could cut tissue which leads to the wound opening. Practice in avoiding too much tension leads to the successful use of finer gauge materials.
The following case study illustrates what happens when sutures are overtight.
Case study
A 56-year old Caucasian male presented with a recurrent basal cell carcinoma of his scalp. The lesion was incompletely removed by a general practitioner six years previously, and subsequently excised by a dermatologist twice – but recurred again. Although basal cell carcinoma may be considered a very “innocent type of cancer” because it rarely metastasizes, it is notorious for recurring locally.
The patient was then referred to a plastic and reconstructive surgeon who booked the patient for a more radical excision of the 10 x 12 mm lesion.
A couple of days later the lesion was removed under sedation in O.T with about 1 cm clean margins making the defect about 2 x 3 cm. The adjacent tissue was undermined for a reasonable distance and closed primarily with 3-0 monofilament resorbable suture material.
The wound appearance at different stages:
Scalp wound after 2 x 3 cm excisionWound 4 days post-operativelyWound dehiscence (10 days post-op)
The wound was initially treated with a topical antibiotic ointment and dressed – but later allowed to dry. Initially, the healing progressed according to plan – but about seven days post-operatively, one of the sutures snapped. The patient reported that: “it sounded like a guitar string snapping in his skull – ZINGGGG.”
On inspection, the wound started to open up and dehisced quite severely. It was decided to allow the wound to granulate and thus heal by secondary intention.
Complications are unpleasant to anyone involved in this kind of a situation, but specifically so to the practitioner and the patient. However, as you may notice, it is not always a train smash. In this case, the wound eventually healed rather nicely with an acceptable aesthetic result.
In the imagines, you will note that the red color marking the dehisced wound fades almost entirely in time as the final stages of wound healing occur and scar maturation progresses.
Discussion
The surgeon opted for a primary closure but may have considered using:
A free skin graft – In my opinion, this would have given a much worse aesthetic outcome. But if the defect was anything more substantial, the surgeon may have had to use this option. Should this procedure be selected, the donor site should be kept in mind since it becomes a secondary surgical site with all the possibilities of complications developing.
A local pedicled scalp flap – This may have been a better choice because the defect margins could be increased. This option minimizes the tension on the wound margin since it “spreads” the wound defect more evenly over a larger area.
Alternative suture materials and techniques – The surgeon could have undermined the wound edges even more and then used a deep layer of resorbable and non-resorbable sutures on the surface for the final closure. This choice gives the surgeon control over the length of time to keep the suture in place. Vertical and/or horizontal mattress suture may have been a better suturing method to use as it would have added a bit more “hold” to the wound closure.
Retrospective wisdom is valuable because it allows for evaluation of choices made – what worked, what didn’t, and what could have been done differently. In my opinion, the surgeon achieved an acceptable and reasonable functional and cosmetic result.
Placement of sutures in an infected wound
Three goals comprise proper wound management.
Provide for a favorable environment for hemostasis.
Prevent any infection.
Arrive at a scar that is aesthetically acceptable.
Infection is a crucial consideration when treating wounds, and all wounds are considered to be contaminated since underlying tissues have been exposed to outside conditions that generally thrive with bacteria. Sutures should not be applied to infected wounds. Suturing wounds is about closing the dead space between severed tissue walls so that they can undergo the natural process of hemostasis. If infected wounds are sutured, or wounds are sutured without being thoroughly cleaned and debrided, an infection will grow and spread, compromising the healing process. Therefore, any infection must be effectively treated before the sutures are applied.
Misplacement of sutures
The most common cause of wound dehiscence is placing sutures very close to the wound edges. Experimental studies show that the more distance there is between the lips of a wound and the suture, the lesser the chances of wound dehiscence. This is because the lip or edge area of the wound displays inflammatory changes, swelling, increased blood supply and reduced collagen structure. The introduction of collagen fibers during the healing phase also puts pressure on the surrounding area, thereby increasing wound tension. Finally, necrotic tissue and aponeurotic tissue zones within the area can also affect suture hold.
Adoption of incorrect suture technique
If the wrong suture technique is used, it can create wound complications such as infection, improper healing, circulation issues, or puffy, broad, or dark scars. Suture breakage is one of the most common problems when improper suture techniques are used. Breaks in sutures can occur due to inappropriate materials, irregular application angles, improper suture material or suture size, and excessive suture tension.
There are eight basic suturing techniques.
Line of interrupted sutures.
Running suture line.
Running locked suture.
Vertical mattress suture.
Pulley stitch, type 1.
Far-near near-far modification of vertical mattress suture, creating pulley effect.
Improper suture techniques can also lead to infection by allowing bacteria to enter the wound. Infection can compromise the healing process and even require that the wound be reopened for cleaning.
Removal of sutures too soon or too late
For a wound to heal properly, it must be assessed and treated correctly. This involves proper cleaning, debridement, and suturing of the wound. Part of the healing process includes applied sutures being removed at the right time which can vary depending on the stress placed on the wound and where it is located. Although the specific situation determines when sutures are removed, they are customarily taken out between 5 to 14 days. If sutures are removed too soon or are allowed to remain too long, complications may arise.
Removing sutures too soon
Sutures are applied to close a wound to keep bacteria out and to allow tissue colligation. If sutures are removed prematurely before underlying tissues have bonded sufficiently, then the wound could reopen (dehisce), damaging newly colligated tissue and allowing bacteria to enter. Deep wounds are particularly vulnerable to dehiscence if they do not have adequate absorbable sutures buried in the underlying tissues providing more tensile strength to hold the wound together.
Removing sutures too late
There are several problems which can arise from sutures being left in too long. First of all, because sutures are looped around wound edges, scar tissue can begin to form around them if they are left in too long. Also, scarring of the wound closure as well as “railroad tracks” from the sutures themselves can be excessive if the sutures remain past the prime removal time. This can be quite problematic if the laceration is in a sensitive area such as the face – therefore, in most cases, facial sutures are removed no longer than five days post-operatively.
The risk for keloid scar formation is also increased when sutures are allowed to remain for too long a period. Keloid scars consist of firm tissue that is much larger than that which forms normal scar tissue and are common occurrences in wounds of the chest, waist, shoulders, elbows, arms, and ears.
African Americans and those having a history of keloid scarring must have their wounds monitored closely so that sutures can be removed promptly to reduce keloid formation. The risk of keloid formation is also higher if the wound dehisces due to premature removal of sutures. It is difficult to be precise on timing, which is why diligently watching the healing process is vital if keloid formation is to be avoided.
The existence of foreign object in the wound
Any wound should be thoroughly cleaned and, if necessary, debrided to remove all foreign material from it. Foreign objects may include wood or metal splinters, glass shards, bone fragments, thorns, gravel, hair, cloth fibers, etc. If external items are not detected during the initial assessment, and the wound is closed, they can present problems such as bleeding, inflammation, infection, and excessive pain.
It is far better to remove all foreign materials during the initial assessment and before closing the wound because objects are more visible. Once a wound is closed with foreign material sutured inside, problems such as inflammation, granulation, infection, and scarring may occur.
Signs of embedded foreign objects
Quite often, patients can feel if a foreign object is present during the initial treatment of wounds. If this is the complaint, providing a more thorough assessment at that time may be beneficial to the patient. However, if foreign bodies are missed and remain in the wound, the following signs/symptoms will ensue:
Local inflammation.
Impairment of healing.
Pain.
Bleeding
Bruising
Persistent draining of an inflammatory exudate or pus.
If signs of remaining foreign objects occur after a wound has been sutured closed, the clinician may opt to use special investigations like X-rays, MRIs and CT scans to assess for the presence of foreign material remaining in the wound.
The longer the object remains in the body, the more it incorporates ingrowth of tissue. An abscess can form, and fistulas may develop between organs. The foreign body reaction may be immediate or may be delayed for years. Diagnosis is sometimes difficult and costly, and removal of the object usually requires major surgery.
Retained sponges can be removed through laparoscopic surgery if they are discovered before adhesions develop.
Determining if foreign bodies should be removed
Once a foreign body is detected, a determination is made if it should be removed at all. If more damage will occur by removing it, the decision may be to leave it in. Other times foreign objects can be removed rather easily. In other cases, the body may dissolve, absorb or expel them naturally over time.
Case study
A 45-year old male presented with vegetative material extruding from a laceration at the superior orbital rim. He had sustained a mechanical fall into a bush three months before presentation. He arrived at an outside ED, where the laceration was repaired. His exam revealed a well-healed periorbital laceration and 20/20 vision on the Snellen chart. A CT scan showed a linear foreign body with its proximal end in the medial orbit.
This object traversed the medial orbital wall, ethmoid sinus, and sphenoid sinus. A dehiscence of the posterior sphenoid sinus wall was noted adjacent to the posterior edge of the foreign body. A CT-A confirmed that there was no apparent injury to the carotid artery. Due to the risk of vascular injury, the procedure was performed in the IR suite. Given the proximity of the foreign body to the carotid artery, an angiogram and balloon occlusion test were completed before the attempted removal and a sheath was kept in place.
A combined endoscopic and open approach was performed by the ophthalmology and otolaryngology services department. A septoplasty with posterior septectomy, left total ethmoidectomy and bilateral sphenoidotomy was required to expose the object. Following this, the team was able to see a stick entering the ethmoid sinus at the lamina paprycea and extending to the right lateral sphenoid sinus. Next, a periorbital incision was made, and dissection was performed along the medial orbital wall until the stick was encountered.
The object was then able to be removed by grasping its proximal end in the orbit and pulling it out. The patient had no neurological deficits postoperatively and was discharged the following day.
Formation of a large blood clot (hematoma)
Uncommon hereditary coagulation disorders can lead to wound dehiscence. In the first month after transplantation, most infections are caused by the same hospital-acquired bacteria and fungi that infect other surgical patients (e.g., Pseudomonas sp causing pneumonia, gram-positive bacteria causing wound infections).
The most significant concern with early infection is that organisms can infect a graft or its vascular supply at suture sites, causing mycotic aneurysms or dehiscence.
Presence of arterial bleeds
When arterial bleeds exert immense pressure inside the wound, it opens. Bleeders are controlled either by ligation (typing bleeding vessels off), or diathermy (burning them closed with an electric current).
Insertion of sutures in a malignant tumor
One of the attributes of a cancerous growth is the loss of cellular adhesion. Sutures placed in a malignant tumor prevent healing.
Prevention
Wound dehiscence may be prevented by taking the following measures [2]:
Avoid unnecessary stress or strain to wound area such as heavy lifting, exercise, vomiting, coughing, or constipation.
Brace the body with a hand or a pillow at the wound site to relieve stress to the wound when doing an activity.
Comply with the doctor’s post-operative instructions and prescribed medication.
Employ wound care, dressing, cleaning and hygiene as prescribed by the doctor.
Maintain good hydration and a healthy diet which can lead to faster healing and prevention of constipation.
Know how wounds normally heal [3]
A normal healing process after surgery can be divided into three stages.
Stage One:
Lasts one to six days.
There may be redness and swelling.
The wound may feel warm and slightly painful to the touch.
Stage Two:
Lasts four days to a month.
A scar begins to form.
Edges will pull together and there may be some thickening. There may also be some red bumps inside the wound site.
Stage Three:
Lasts six months to two years, depending upon the type of surgery.
Wound fills in and a new surface is present.
Scarring becomes thinner, flatter, and whiter.
Any deviations from this healing process, particularly between five to ten days postoperatively, could indicate possible dehiscence. Most dehiscences occur four to fourteen days after surgery. Contact your healthcare professional if there are any concerns about the healing progression.
Be proactive and prepared
Left untreated, wound dehiscence can lead to more serious or life-threatening conditions. By understanding the healing process and being attentive to it, you’ll recognize if it’s falling outside typical parameters. Then you can get in touch with your healthcare provider for early intervention. Through this simple, proactive measure, you may avoid dehiscence and contribute to an optimal healing outcome.
Today we present an interview with Leann Williams, a surgical technologist and surgical technologist educator from Tucson, Arizona.
What makes surgical technologists special?
“We are one of the only healthcare professionals who get the opportunity to hold a beating heart, touch the brain; not just a mind, and bring life into this world.”
How did you first get interested in Surgical Technology?
“I wanted to be in the healthcare field as a young adult. After watching MASH, (a television show popular back in 1972-1983 about a Mobile Army Surgical Hospital ) I knew surgery was for me. I walked into the school 26 years ago and have never looked back with regret. I absolutely love this profession.”
How wonderful that you enjoy the position as much today as you did when you first started. That’s rare. Tell, me, how long did it take to earn your degree?
“It didn’t take too long. I graduated with a Diploma in one year.”
Just a year and you were practicing. That’s good news for many of our readers who want to be in a healthcare profession, but want to get into the field as soon as they can. While you were in school, what was your favorite part of the surgical technology program?
“My favorite part of school was learning, thinking about the possibilities of the profession and knowing I would be making a difference in people’s lives. I feel the same way about being a surgical technologist.”
While you were in school, was there a course you found more difficult than other courses?
“Anatomy was hardest for me. Suturing can also be a difficult skill to learn.”
I can see how those two courses would be difficult. Our readers may be seriously considering entering school for surgical technology. If they make the decision to do so, what is the most important thing they need to remember while enrolled in a program?
“I would tell them three things. Never give up; the word “no” means try again; and tomorrow is a new day. Those three concepts become a philosophy to get you past days when the program feels overwhelming.”
You’ve been a surgical technologist for a while. Is there a type of surgery you like better than others?
“I like brains, big open vascular procedures, orthopedics, and general surgery. I have to confess that I don’t like teeth and eye surgeries make me cry.”
Thank you for sharing that. I think eyes would make me cry, too. In our surgical technology article series, we share that a person can become a surgical technologist, and then move on to become a surgical first assistant. What’s the difference between the two? Do you recommend one over the other? Is there any advantage of being one or the other?
“I’ll try to break this down. The first step everyone has to take is graduating from an accredited surgical technology program and to get some experience. Then, if you want to assist in surgery, you would apply to an accredited first assist program.
The opportunities as a first assist are different because you can do more. Career options are also broader. You can work for a hospital, a surgeon, or be self-employed. Reimbursement qualifications are different in each state.”
Thank you for explaining this and helping us understand you have to be a surgical technologist before becoming a first assistant. Do you recommend becoming a Certified Surgical Technologist; a CST?
“I always recommend taking the CST exam and remaining current in this profession. Being a CST helps to promote the profession by letting the community know you have gone the extra mile, followed by continuing educational credits to remain current. CSTs are hoping that all states will adopt certification as a requirement of employment.”
In talking with you before the interview, you shared with me that sometimes a surgical technologist can become a permanent part of a team. How difficult is it to become a regular or permanent member of a surgical care team?
“Educators always hope the hospital where the extern (clinical) is performed, that employment will follow. Just like any other profession, if you are not motivated to work, you will not be offered a job.”
Thanks. Can you tell our readers what is a common misperception people may have about surgical technology as a career?
“That’s a good question. Most people think that all we do is pass instruments. We do much more than that. We know anatomy and apply the knowledge of instrumentation and equipment to surgical procedures. We understand pharmacology, patient care concepts, the importance of aseptic technique, decontamination and sterilization of instruments, position, prepping and draping of the patient, and policy and practices around prepping products for the safety of the surgical patient”
That’s quite a bit of responsibility. I can see why a degree, and a CST are important. Can you share with us any one thing to always keep in mind when you’re a surgical technologist involved in an active surgery?
“Never forget that no matter what condition the patient is in, they were/are someone’s baby. Remember to always treat each and every patient as you would want your own baby/mother/family member treated. Everyone is someone’s VIP.”
I think that’s very true and thank you for reminding all of us about that. Can you tell us if there is anything a person still in high school can do to prepare to become a surgical technologist?
“I recommend making an appointment with the program director of a surgical technology program. Interview that person and see if they inspire you to be more. Watch YouTube videos of different surgeries, talk to surgeons, visit the school, and talk to their students. Always make sure you have a passion to make a difference.”
As a surgical technologist yourself, what is the most challenging aspect of the profession? And the most rewarding?
“One of the most challenging aspects is death. Members of surgical teams invest so much energy that when a patient passes, we all have to walk through the stages of grief. Death always has an impact and while you may never get used to it, you do have to accept it as part of the profession.
The most rewarding is having the opportunity to see a person, who is your patient, like no one else has. We see them inside and out, literally. It’s a huge honor to have the trust of patients and their family members.”
Medical technologies, techniques, and even approaches change almost daily. What advancements in surgical techniques and equipment do you see?
“The first thing is Robotics (DaVici). They are being used for more procedures. I also see more efficient surgeries. Surgeries that in the past took four hours are now taking approximately 30 minutes. The equipment is advancing to make dissection easier. All of this promotes better care for patients.”
A question related to this is about the machines in an OR. Our previous articles have mentioned that sometimes surgical technologists have to make sure machines are in good working order. Is it hard to learn what all the machines in an OR do?
“This is like any new job. It takes practice and repetition, which is why there are so many clinical hours involved in surgical technology education programs. Continuing education also keeps you abreast of anything new you may need to know about or get comfortable with.”
You referred to continuing education. What types of continuing education credits have you obtained over the years?
“I attend theAssociation of Surgical Technologists(AST) National Conference, instructor forums, state AST workshops, online CEU offerings. As your readers may know, maintaining aCSTrequires 60 CEUs over four years. If someone advances to a first assistant, that license, aCertified Surgical First Assistant(CSFA), requires 75 CEUs over four years.”
I appreciate your patience with all these questions. I promise we only have a few more. How long would you say an average operation lasts?
“Length is determined by the type of surgery needed, and if any complications arise. Surgeries can be as short as ten minutes or as long as eight hours.”
Our previous articles on surgical technology mention that surgical technologists are members of a surgical care team. How many members are on such a team?
“For a typical case, members of a care team include a surgeon, an assistant (physician assistant, certified first assistant or medical doctor), an anesthesiologist, a surgical technologist and a registered nurse. For a heart procedure or larger case, there may be additional surgical technologists and registered nurses.”
This is the last question. I know there are unique sights and sounds and even odors in an operating room that the average person doesn’t normally encounter. Did you have to get used to all that?
“This question brings me to a story about when I first started. I was still in school and went for an observation day in the operating room. My very first surgical procedure was a laminectomy (a procedure that enlarges a spinal canal in order to relieve pressure on the spinal cord or nerves). They brought the patient into the operating room and promptly removed the blanket, exposing the patient’s completely naked body. I quickly turned around and counted the tiles on the ceiling behind me. So, to answer your question, yes, I had to get used to all kinds of things. But eventually I did and realized that smells and patients aren’t like Christmas presents. It doesn’t really matter what’s on the outside. They are all the same on the inside.”
Thank you so much for your time today. I know the insights and information you’ve shared today will help our readers know if this is the career path for them.
Leann Williams is currently the Program Director of the surgical technology program atPima Community Collegein Tucson, Arizona. Her program currently maintains above an 85% passing rate on the national certification for surgical technologists. Before entering the field of surgical technology education, Ms. Williams worked as a surgical technologist for over ten years at Northwest Medical Center and over 11 years at Tacoma General Hospital.
Get Started on Your Path of Surgical Technology Today
Ms. Williams shared with us that the skill of suturing may be difficult to learn. If her interview has sparked your interest in becoming a surgical technologist, why not get a head start on your own suturing skills? You can do so through The Apprentice Doctor. We offer asuturing kit, complete with instructional videos, where you can practice suturing, tying knots and other skills common in the field of surgical technology. As you gain agility in performing these critical tasks, your confidence in pursuing this career will grow. More importantly, after completing this internationally accredited program, and talking to a surgical technologist program director as Ms. Williams suggests, you’ll know if surgical technology is the field for you.
If you missed any article in our surgical technology series and would like to go back and catch up, click on the following links:
If, after becoming a certified surgical technologist and working in the field for a period of time, you may want to advance in this allied health career. If this sounds like you, investigate becoming a Certified Surgical Assistant (CSA), or Certified Surgical First Assistant (CSFA).
Surgical assistants are medical professionals who assist both surgeons and nurses during surgical and other medical procedures. Like surgical technologists, they have specific responsibilities in the operating room, plus pre- and post-surgery duties.
A first assistant position is not an entry-level position. Because it is the next level up in skills and leadership, you must already work in the healthcare field as a surgical technologist, nurse or other health professional, preferably in a surgical capacity.
What does a surgical assistant do?
The primary duty of surgical assistant is assisting surgeons. You’re under their supervision when performing all tasks.
Typical duties include:
Administering needles.
Closing surgery sites.
Collaborating with doctors, consultants and other surgical team members to ensure the proper post-operative care of patients.
Controlling bleeding.
Dressing wounds.
Monitoring electronic medical equipment.
Performing minor surgical procedures.
Positioning and prepping patients prior to surgery.
Resuscitating patients.
Responsibilities of a surgical assistant can be broken down into four different areas which align with most surgical assistant education programs.
Preoperative
Facilitate positioning of the patient, taking into consideration:
Patient’s anatomical and physiological limits.
Surgeon’s preference.
Surgical procedure to be performed.
Surgical site.
Assist circulator and anesthesia provider in some of the following ways:
Catheter placement.
Tourniquet application.
Other procedures as needed.
Intraoperative
Perform specific tasks utilizing appropriate techniques.
Achieve hemostasis by means of injection.
Aide in implanting, securing, and/or removal of devices and drains.
Apply appropriate dressing material(s).
Incision and layered closure of surgical sites.
Manipulation and dissection/removal of tissues.
Postoperative
Aid in transfer of the patient.
Apply specific dressing material such as splints or casts.
Assess skin integrity.
Follow patient to recovery as needed.
Specialty Procedures
With appropriate training and supervision:
Graft and implant preparation.
Vein and graft harvesting,
The responsibilities of a surgical assistant help surgeons perform safe operations resulting in optimal results for the patient. Tasks are more expanded and elevated than those of a surgical technologist. The pressure is also higher, so when considering this professional career, you will have to decide if you want to deal with this type of stress on a daily basis.
Work environment
The work of a surgical assistant is every bit as physically demanding as that of a surgical technologist. You’re on your feet most of the day, and are expected to stand throughout all procedures regardless of length. You must always be attentive, anticipating what tools the surgeon may need and respond quickly when she or he asks for them.
Like surgical technologists, surgical assistants wear scrubs to minimize the possibility of infection to the patient. And similar to all members of a surgical care team, jewelry and long nails (even artificial nails) are almost always prohibited.
As a surgical assistant, if you have an entrepreneurial nature, you may decide to be self-employed. You can also work in hospital surgical units, surgery centers or private surgical medical practices. If you enjoy teaching others about the profession, you can also become an academic instructor.
Hours
Almost all surgical assistants are hired as full-time employees. Hours and weeks are long depending upon the number of surgeries scheduled in any given day or week. If you go into this career field, expect early morning hours, being called in to assist with emergency surgeries, and working on holidays and weekends.
Required education
In all cases, to become a surgical assistant you’ll need to graduate from an accredited surgical first assistant program.
In most cases, in order to enter a surgical first assistant program, you must first have an associate degree in surgical technology from an approved, accredited surgical technology program. You must also have successfully passed your Certified Surgical Technologist (CST) exam conducted by theNational Board of Surgical Technology and Surgical Assisting(NBSTSA).
Some surgical assistant programs may also require one or more of the following:
Several years of experience in operating room assisting (often must be completed within the last 3-5 years).
Proof of a current CPR certification for healthcare providers.
Updated immunization records.
Certain course work such as physiology, microbiology and/or medical terminology (taken within the last 7 years).
Check the admissions guidelines of the surgical assistant program you are interested in. Once you find the right educational program for you, it can be completed in as little as 12 months.
The overall objective of most surgical assistant programs is ensuring students can perform surgical assistant skills with proficiency. The curriculum provides students with the experiences necessary to document 135 or more procedures, all designed to verify competencies required of the position.
Specific program objectives will meet standards established by the various approval and accrediting organizations.
Most will be similar to the following:
To provide a competency-based environment where students can apply their advanced knowledge of normal and pathological surgical anatomy and physiology.
To deliver a training program in various settings where students can demonstrate preoperative, intraoperative and postoperative skills.
To offer students opportunities to acquire and practice professional behavior in working relationships with patients and members of a surgical care team.
To ensure students are able to communicate patient needs and surgeon preferences to all members of a surgical care team.
To facilitate the professional leadership growth of students through knowledge of the role and how it pertains to ethical, moral and legal responsibilities.
Surgical assistant programs are carefully sequenced between clinical experiences, and classroom theory. Although you will have assisted in many procedures as part of your surgical technology degree and experiences, the clinical cases in a surgical assistant program involve utilizing more skills. The variety and intensity will be different than what you’re used to.
The concentration curriculum of most surgical assistant programs is comprised of advanced courses in surgical technology. Although you may have taken similar courses in your associate degree program, surgical assistant courses go into much more detail.
Programs may be separated into specific areas and look something like this:
Healthcare Sciences
Microbiology
Pathology
Pharmacology
Technical Sciences
Information technology
Robotics
Surgical Technology
Case management
Intraoperative duties
Preoperative duties
Postoperative duties
Surgical Speciality Procedures
Gynecology
Obstetrics
Orthopedic
Neurosurgery
Plastic and Reconstructive
Clinical rotations (135 or more procedures plus observation of many more)
Graduates of a surgical assistant program can then become Certified Surgical First Assistants (CSFAs) or Certified Surgical Assistants (CSAs). Each credential is offered by a different organization and has different eligibility requirements.
Both of these exams are standardized tests that prove you possess the appropriate level of education, experience and skills to be a trusted surgical assistant. Passing one is required in order to work as a surgical assistant.
Certified Surgical First Assistant (CSFA) credential
Currently the test is composed of nine graded, multiple-choice questions and you must correctly answer a specific number of them to pass. All applicants for the exam must be graduates from a CAAHEP-accredited training program. In the alternative, with documentation of appropriate work experience, continuing education and certification, this requirement may be waived.
Eligibility Table
Status
Documentation Needed
Other Items to Include
Graduate of surgical first assisting program –CAAHEPapproved
Evidence of graduation through one of the following:
• Notarized letter on institutional letterhead from program director or registrar (name, date of graduation, type of degree awarded); OR
• Copy of graduation certificate/diploma or transcript.
• CSFA exam application
• Appropriate fee
Currently certified Surgical Technologist (CST) who can demonstrate appropriate experience
• CST credential
• Verification forms from sponsoring agencies for:
• 200 cases (75 general surgery; 75 in one speciality area; 50 in any other speciality area(s)) within 2 years prior to application date & during a pre-approved timeframe.
• CSFA exam application
• Pre-authorization form
• Evidence of malpractice coverage
• Appropriate fees
Graduate of military surgical technology training program
Verification forms or case log(s) for:
• 200 cases (75 general surgery; 75 in one speciality area; 50 in any other speciality area(s)) within 4 years prior to application date.
• CSFA exam application
• Evidence of graduation (ex. DD214) and/or completion certificate)
• Appropriate fees
Current Certified Surgical Assistant (CSA)
• CSA credential
• Verification forms or case log(s) from sponsoring agencies for:
• 200 cases (75 general surgery; 75 in one specialty area; 50 in any other specialty area(s)) conducted within 2 years prior to application date.
• 50 continuing education credits within 2 years prior to application date.
• CSFA exam application
• Continuing education reporting form
• Appropriate fees
Once your application is approved, NBSTSA sends you an Authorization to Test number (ATT) and a phone number/web address for an approved testing agency. You will schedule your exam with that agency. The entire process takes 4-6 weeks to complete.
Remember, if the surgical assistant program you are considering is not CAAHEP-accredited, obtaining the CFSA credential may prove difficult. The CFSA is the credential most employers look for.
All applicants for the exam must be graduates from a NCCSA-approved training program which is accredited by either CAAHEP or the Accrediting Bureau of Health Education Schools (ABHES). With appropriate documentation, there are some alternatives to this, such as military training, that may be used in lieu of this requirement. Check the NCCSA website for the specific documents you may need you’ll need for your status.
Eligibility Table
Status
Documentation Needed
Other Items to Include
Graduate of surgical first assisting program NCCSA approved AND either CAAHEP approved or ABHES approved
• Evidence of graduation
• Proof of formal training
• CST credential
• Experience affidavit
• Skills affidavit
• 3 letters of recommendation from surgeons you assisted
• Verification of one year of case logs proving you were the primary assistant in at least 2250 procedures within the last 3 years.
• CSA exam application
• Appropriate fees
New graduate (within last 12 months) of surgical first assisting program NCCSA approved AND either CAAHEP approved or ABHES approved
• Evidence of graduation
• Proof of formal training
• CST credential
• Experience affidavit
• Skills affidavit
• 3 letters of recommendation from surgeons you assisted
• Verification of one year of case logs proving you were the primary assistant in at least 2250 procedures within the last 3 years.
• CSA exam application
• Appropriate fees
Active military surgical training
• Evidence of graduation
• Proof of formal training
• CST credential
• Experience affidavit
• Skills affidavit
• 3 letters of recommendation from surgeons you assisted
• Verification of one year of case logs proving you were the primary assistant in at least 2250 procedures within the last 3 years.
• CSA exam application
• Appropriate fees
Once your application is approved, within 48 hours you will receive a phone call to schedule your testing date.
Required continuing education and renewal certification
Like with most professions in allied health, surgical assistants are required to take additional courses once they are certified. Depending upon the type of certification you have, the renewal criteria is different.
CSFA Renewal
Every four years, the NBSTSA requires 75 credits of continuing education for CFSA renewal. Proof of these 75 credits is submitted with your renewal application. If you happen to hold both a CST and a CSFA, when you complete 75 credits, both credentials can be renewed. Details, steps for renewal, and updates are always located on the NBSTSA site.
Eligibility Chart
Option 1
Option 2
Other Items to Include
Documentation of 75 continuing education credits earned within the 4-year cycle
Retake the CSFA exam, meeting all the initial requirements
• CSFA renewal application
• Appropriate fees
CSA Renewal
If you possess a CSA, you are required to complete 50 CSA credits within your two-year certification period. Details, steps for renewal, and updates are located on theirwebsite.
Eligibility Chart
Option 1
Option 2
Other Items to Include
Documentation of 50 continuing education credits earned within the 2-year cycle
Retake the CSA exam, meeting all initial requirements
• CSA renewal application
• Appropriate fees
Fees and deadlines for certification and renewal
Regardless which certification you opt for, following the eligibility requirements exactly is important or there will be delays in obtaining your certification or renewal. Without it, you may be unable to practice in the field. In the case of renewal, if you allow your certification to lapse, you may be suspended from practice until your renewal is taken care of.
Take your first-time certification exam as soon as possible after graduation. Bear in mind that while your education is extensive, it will not be enough to pass the test. Purchasing a study guide or registering to take a qualified review course immediately prior to the exam will improve your chances of passing the test.
Apply for renewal two to three months prior to the expiration of your current certification. Be sure you have participated in continuing education credits throughout the period of your certification. You will be unable to secure all the necessary hours in a short period of time. When sending in your documentation, always keep copies.
Fees for certification and renewal range from $100 to $700. If you are a member of a surgical technology support association (ASA or NSAA), fees for these tests are normally reduced. The CSFA test recognizes membership in theAssociation of Surgical Assistants(ASA). The CSA test recognizes membership in theNational Surgical Assistant Association(NSAA). Proof of your membership is required. More information on these two organizations is located at the end of this article.
Job outlook
TheBureau of Labor Statistics(BLS) indicates the demand for surgical assistants will rise 12% through 2026. People are healthier than ever before, and they are living longer. However, 60% of the senior American population suffer, on average, from at least two chronic illnesses. So the demand for all healthcare professionals is high. For more statistics and estimates of annual salaries, you can visit the BLS.
General skills needed for a surgical assistant
To be a successful surgical assistant, there are essential technical skills you’ll need beyond those required of a surgical technologist. In hiring situations, employers look for the following primary competencies:
Ability to correctly respond to orders – You have to cheerfully follow orders precisely and immediately.
Effective communication skills – You must be able to communicate all types of information to patients and members of a surgical care team.
Handling high-pressure situations – Due to the intensity levels in an operating room, you must be able to react intuitively in short time frames.
High attention to detail with a long attention-span – Attentiveness to anything abnormal in a patient’s vital signs is essential.
Personal fitness – You have to lift and reposition patients, so a certain level of fitness is beneficial.
Self-confidence – Pre- and post-surgery procedures are frequently performed alone, so you have to possess enough confidence to do them and know you’re doing them correctly.
Strong hand-eye coordination and dexterity – Surgical work involves both large and small surgical procedures. A surgical assistant must be able to assist with both.
Wide range of personal and professional skills – This encompasses technical skills inside the operating room and leadership skills outside of it.
Working both independently and in a team environment – You must be comfortable working with peers as well as people in positions of authority. Outside of the OR, you will be expected to work on your own when following up with patients.
3 reasons to become a surgical assistant
Work with the latest technologies
Many surgical assistant programs provide some robotic surgical procedure training. The workplace may expose you to others. Opportunities to remain current with the most recent advances that minimize risk to patients and speed up recovery time can be exciting.
Learn something new daily
Although you acquire a lot of education when becoming a first assistant, you’ll learn even more from members of your surgical team. The more you know, the more valuable you are.
Work with a team
Working in an operating room is demanding. Team members of a surgical care unit are no less so. Collaborative team membership adds to your leadership and technical skills.
Surgical assistant organizational support
As a surgical assistant, or even a surgical assistant student, you can join theAssociation of Surgical Assistants(ASA). This organization supports people in the profession, and those aspiring to the career. It works toward ensuring optimal surgical patient care. It also promotes the recognition of surgical assistants and offers continuing education opportunities.
You may elect to become a member of theNational Surgical Assistant Association(NSAA) on their site. They promote excellence in the field, offer educational opportunities and professional certification, and encourage the recognition of surgical assistants.
Want to start now?
Even if you are still in high school, if you are interested in the field of surgical assisting, you can begin today by acquiring a suturing kit.
The Apprentice Doctor offers these kits, complete with instructional videos. You can practice suturing, tying knots and other skills common in the field. As you’ve learned, you need a lot of self-confidence as a surgical assistant. With a suturing kit, you can begin growing that confidence as you gain agility in performing critical suturing tasks. After completing this internationally accredited program, you’ll possess advanced skills and knowledge in the field.
If becoming a doctor isn’t the right career for you, but you would like to work in allied health, surgical technology may be a good option. Surgical technologists work alongside doctors and surgeons. They are frequently present during operations and provide critical assistance to operating room physicians.
What does a surgical technologist do?
The primary duty of surgical technologists is assisting surgeons during surgical procedures. They prepare operating rooms, arrange equipment, and even help in post-operative recovery rooms.
Typical duties include:
Preparing patients for surgery.
Transporting patients to and from operating and recovery rooms.
Sterilizing equipment and ensuring adequate supplies for surgery are available.
Passing surgeons instruments and other sterile supplies.
Maintaining a sterile environment.
Providing tools and suturing wounds for surgical team members.
Observing and reporting patients’ vital signs.
Organizing paperwork documenting any surgical procedure.
Utilizing medical tools.
Surgical technologists are important members of surgical teams, especially since technologists are responsible for many preparatory tasks relating to surgeries. For example, you may be asked to prepare an operating room. This can range from setting up trays of instruments in a sterile field to preparing patients for surgery. Because you’ll know how medical equipment works you may be required to ensure all surgical machines are working properly. You will be familiar with these tasks since they are all part of a surgical technology education.
Your job duties don’t end at pre-operative care. When watching medical shows on television, you have probably seen individuals pass instruments and supplies to surgeons during an operation. Surgical technologists are frequently the individuals who do this. You may also be asked to hold internal organs in place while the surgeon operates. In some cases you may handle specimens taken for laboratory analysis.
At the conclusion of an operation, surgical technologists dress incision sites. You may be asked to take patients into a recovery room and observe them until they come out of anesthesia. Restocking operating room supplies after a procedure may be one of your responsibilities.
Duties vary from day-to-day, and sometimes hour-to-hour. It’s an exciting field with many possibilities for personal and professional growth.
Work environment
The work of a surgical technologist is physically demanding. You’re required to remain standing throughout the entire surgical procedure. Some operations are short. Others can be as long as eight or ten hours. You must be alert and constantly aware of what is happening around you for the duration of the procedure.
Being comfortable with the sight of blood, bones and internal organs is essential. You must be equally comfortable holding living organs inside a body cavity of a patient. In addition to these sights, you are exposed to unpleasant odors and possibly communicable diseases. While all precautions are taken, there is always some risk when performing this kind of a job.
Surgical technologists wear prescribed clothing called scrubs. Scrubs are special sterile clothing operating teams must wear to minimize the possibility of infection to the patient. Depending upon where you work, specific colors and types may be required. As part of this dress code, jewelry, long nails (and even artificial nails) are almost always prohibited. The risk of an earring, or acrylic nail falling into an open body cavity is too great, so this requirement is a typical standard of care.
Places you can work include hospital surgical units, ambulatory surgical centers, free-standing out-patient surgery centers or private surgical medical practices.
Hours
Although surgical technologists can work part-time, most are hired as full-time employees in hospitals and clinics. Where you work determines hours and shifts. However, since many surgeries are performed in the mornings, your day may start as early as 5:00 a.m. Hours fluctuate depending upon the daily and weekly operating room schedule. You can be called in at the last minute to assist with an emergency operation.
You may also specialize in a type of surgery, such as cardiovascular, and become a regular member of a surgical team. In those cases your hours may be a little more predictable, but they will still be long (over eight hours a day) and rigorous. Surgical technologists will have rotations where they are on call during nights, weekends and holidays.
Required education and certification
In most cases, to become a surgical technologist you’ll need some kind of a degree from an accredited surgical technology program. Graduates of these programs can then become Certified Surgical Technologists (CSTs). The CST exam is a standardized test that helps employers know you have the skills and knowledge necessary to be a capable and trusted surgical technologist.
The CST test is conducted byThe National Board of Surgical Technology and Surgical Assisting(NBSTSA). Their website provides comprehensive information about the exam, practice tests, and eligibility requirements. Although some employers don’t require certification, most do. In all cases having a CST after your name enhances your employment opportunities.
You can earn a degree in surgical technology in 12-24 months. Most programs are on-ground, although some may be a combination of on-ground and on-line courses. All surgical technology programs require an externship, or internship, of surgical rotations. Practical experience is part of any surgical technology curriculum. The experiential components of the program applies what you’ve learned in the classroom to actual operating room experience. Like doctors, you’ll rotate through different types of surgeries. In these rotations you’ll determine if there is one type of operation you prefer over another.
The objectives of most surgical technology programs are:
To provide a competency-based environment in a classroom using current models and trends in the industry.
To deliver a training program in a setting where surgical technology students can apply the theoretical knowledge gained during the lecture portion of the training to the performance of skills used in an operating suite.
To offer students opportunities to acquire and practice professional behavior in working with relationships with patients and members of a surgical care team.
To facilitate the occupational growth of students by providing access to the knowledge base and applied skills necessary to become an integral member of a surgical care team.
Surgical technology programs are linear. Linear means that with some exceptions, you’re required to take the courses in a certain sequence. Surgical technology courses build upon each other. In other words, you need to know the information in one class to understand the information in the next course and so on.
Most surgical technology programs provide the study of general and specialty surgical procedures. An academic associate degree in surgical technology will include some general education courses like psychology and English composition. An associate degree takes longer to complete. However, the general education courses assist graduates in growing professionally and in developing the ability to assume roles of leadership in the work environment.
The concentration curriculum of most surgical technology programs will consist of the following types of courses:
Medical math and calculations
Medical terminology
Anatomy & physiology
Medical ethic
Clinical procedures (general medical procedures)
Pharmacology for the surgical technician
Surgical technology techniques
Surgical procedures (multiple courses)
Specialty surgical procedures (multiple courses)
Surgical externships (could be 500+ hours of practical application threaded through some specific courses)
Like with most professions in allied health, surgical technologists are required to take additional courses once they are certified. Every four years, the NBSTSA requires 60 credits of continuing education for CST renewal. You will have to provide proof of these 60 credits when you submit your renewal application. Details and updates are always located on the NBSTSA site.
With a surgical technology degree you can obtain employment as a Surgical Technician or Surgical Technologist.
Job outlook
TheBureau of Labor Statistics(BLS) indicates the demand for surgical technologists is rising. This career is expected to grow at the rate of 12% between 2016 and 2026, which a faster pace than other careers.
General skills needed for a surgical technologist
To be a successful surgical technologist there are important technical skills you’ll need.
In hiring situations, employers of surgical technologists look for the following primary skills:
Aseptic – You must understand how to maintain an environment that is free from bacteria and contamination.
Cardiopulmonary resuscitation (CPR) – In an emergency, you may be required to keep brain function intact until an appropriate medical professional arrives on the scene. A certification in CPR is always required and something you’ll obtain as part of your education.
Communication – You must be able to communicate verbally and also on paper (medical records and patient charting). Part of your communication skills include superior listening since care of patients includes knowing how they are feeling.
Computer skills – Many hospitals now have their records on computer. They also record notes and observations in real time on tablets. Knowledge of computers and other technical devices will help you in securing a job.
Organization – In this position you have to keep medical supplies, operating room instruments, and even schedules organized and free from chaos.
Patient care – You must truly enjoy working with people and listening to what they have to say.
Physical demand – The ability to stand for long periods of time is essential. You’ll also be required to transfer patients, so lifting a certain amount of weight is expected.
Sterile techniques – Knowing how to set up, maintain, and remove sterile fields is required.
Surgical procedures – You may be asked about your familiarity with various types of surgical procedures.
Teamwork/collaboration – Surgeries are performed by surgical teams that perform well together. Since surgical technologists are vital members of these teams, you must be able to interact and get along well with team members.
5 reasons to become a surgical technologist
You can enter the field quickly – Surgical technology programs take anywhere from 12-24 months to complete. By researching approved programs, you’re apt to find one that meets your budget and your time frames.
Demand is high – Because an increase in surgical technologists is expected through 2024 (BLS), once you’re a CST, employers will be interested in hiring someone with your skills and credentials. Growth is high due to ongoing advances in surgical technology. These advances mean more surgical procedures can be performed, many with lower risks to patients. A larger, and aging population also contributes to the demand.
You can work anywhere – A CST (Certified Surgical Technologist) is a national certification, so your qualifications move with you. Additionally, since most surgical technologists are hired by hospitals, and hospitals are located throughout the United States, job opportunities exist in most places.
There is a lot of variety – Even if you specialize in a specific surgical technology area, no patient or procedure is ever the same. So your days and weeks will not be spent in repetitive task assignments. Although the pressure is high, some of the uniqueness of your days may be a good offset for you.
You can make a difference in someone’s life – Patients undergoing surgery are usually scared. Since part of your job as a surgical technologist is interacting with patients before and after surgery, you can provide assurance to them. It is also very satisfying to see patients thrive and return to their life interests after a surgery is conducted. As a surgical technologist, you will have contributed to their return to health and lifestyle.
Surgical technology organizational support
As a surgical technologist, or even a surgical technology student, you can join theAssociation of Surgical Technologists(AST). This organization supports people in the profession, and those aspiring to the career. It provides information on technical advances, public policy, and changes in educational standards.
Want to start now?
If this article has sparked your interest, you can begin practicing some of the skills required for a surgical technologist, regardless of your age.
Through The Apprentice Doctor you can acquire a suturing kit, complete with instructional videos. With this kit you can practice suturing, tying knots and other skills common to the field of surgical technology. You’ll grow in confidence as you gain agility in performing these critical tasks. More importantly, after completing this internationally accredited program, you’ll know without a doubt you want to become a surgical technologist.
A specialist surgeon is someone who focuses on a particular field of medicine such as cardiology, neurology, or another specific medical field. All specialist doctors have many years of education and training in their chosen areas. But before you learn how to become a surgeon who specializes in a single discipline, there are preliminary steps you need to take.
First, you will need to become a medical doctor. Becoming a medical doctor requires, depending on the state/country you live in, that you obtain a premedical science degree and follow it up with a medical degree. More often than not, your undergraduate degree will take about four years, and medical school will require another four.
Second, it is beneficial to gain real-world experience for several years as a general practitioner before going into a specific branch of medicine.
Third, you’ll have to apply for admission as a candidate to the training program of the surgical department of a medical school. The admission criteria for a trainee as a general surgeon are strict, and competition is usually fierce. This training could last from five to eight years. At that point, you can become certified in that field of surgery.
What are the attributes that I need to become a surgeon?
Successful surgeons possess specific characteristics and outlooks that contribute to fulfilling careers. Although a strong desire to become a surgeon is paramount, and the tenacity to persevere through ten or more years of formal training is essential, you must possess other attributes as well. Without them, a career in surgery may prove challenging and unrewarding.
In addition to the ability to think on your feet, problem-solve and work well under high levels of stress, you must also be able to manage:
Crises and emergency situations.
Long and grueling hours.
Extended periods of absolute concentration without breaks.
Working with your mind and your hands.
You must also possess:
Physical dexterity. Although you can acquire a certain amount of dexterity through practice, some of it is an innate ability. If you have had difficulty with dexterity throughout your life, surgery may prove difficult for you.
Respect for the human body and human life. Although the field of surgery may provide you with a very comfortable lifestyle, to be successful, your primary motivation must be a love of and respect for the human body and human life. Without it, patients may see you as less than genuine and not trust you.
Love of anatomy. A thorough knowledge of anatomy is the foundation of surgery.
Intelligence. If you struggle with your studies despite putting in effort daily, you may benefit from submitting yourself for psychological assessment to ascertain if you have the intellectual capacity to become a doctor or a surgeon.
Basic Principles Applied in Surgery
Regardless of the surgical specialty, or type of surgery performed, every surgeon applies fundamental principles in the operating room. Because it contains innate properties, human tissue reacts to injuries in predictable ways. So, over time a set of guidelines evolved to promote optimal healing. Commonly referred to as the basic principles of surgery, every surgeon, regardless of specialty or type of surgery performed, follows them in the operating room.
Diagnosis and preoperative assessment. An incorrect diagnosis may result in inappropriate, ineffective and possibly unnecessary treatment.
The consideration of alternative non-surgical treatment modalities. Because most surgery is invasive, it should be the last resort.
Proper treatment planning. It is said that good surgeons always operate twice. They visualize and plan the operation mentally before doing the actual surgery. Assisting the surgeon in this planning process are tracings, computer assisted simulations, model surgery, etc.
Minimum invasion. When possible, consider alternatives to open surgery.
Scope-assisted surgery versus an open surgical procedure.
Interventive radiology/angiography.
Surgical procedures to the heart requiring the opening of the chest are being replaced in some instances by minimally invasive procedures performed by accessing the inside of an artery and performing the relevant procedure with radiographic (X-ray) assistance.
Good visual conditions. Surgeons must be able to clearly see the area they’re working on.
Exposure of the surgical site. This takes place when the surgical incision is made, and dissection is performed to reach the intended surgical site.
Retraction is the “pulling” away of tissue to offer the surgeon maximum exposure to the surgical site.
Surgical assistants and nursing staff have noted that successful surgeons always seem to complain about the light.
Suctioning and sponging. This is necessary to remove excess blood which may obscure the operative field.
Some noted physicians in history were handicapped by blindness, but not so with surgeons.
Handle tissue gently causing as little injury as possible. This amounts to having respect for the human body as well as an understanding of the processes involved in the repair and healing of wounds.
Proper control of bleeding within the limits of:
Minimal electrocautery.
Minimal suturing.
Minimal sponging.
Every action must be purposeful. For safety and economic reasons, in the operating theater, time is of the essence. Do not waste time in the OT.
Sterility and asepsis. All surgical instruments must be sterile (the complete absence of microorganisms), and the operative field must be as aseptic (minimizing and weakening microorganisms) as possible.
Other principles applied are not surgical in nature, but are still critical to patient comfort, trust and confidence.
Anatomical considerations.A surgeon needs to have a detailed knowledge of the structure of the human body.
Physiological considerations. A surgeon must have a comprehensive understanding of how the human body functions.
Patient considerations. It’s critical for surgeons and members of the surgical team to take into account the fears and preconceived ideas of the patient about surgery and its outcomes.
Social.Certain diseases are more prevalent in specific socioeconomic groups than in others.
Religious. The transfusion of blood or transplantation of organs is a taboo in some religious groups.
Financial.What are the economic implications of the proposed operation to the patient/healthcare organization?
Expectations. What is the expected outcome and success of the procedure?
Communication. It is essential the patient understands the parameters, risks, and limitations of surgery and anesthesia. Providing information on scars and other conditions that may be present after surgery is necessary so that the patient is as prepared as possible for the operation and what may transpire when it is finished.
Information. This includes data about the proposed procedure and any alternatives. The patient must also be informed about any potential pain or discomfort that may be experienced, as well given pre- and postoperative instructions.
Implications.Will the patient be able to continue with normal activities e.g., studies/work/sport/hobbies? If not, will the condition be temporary or permanent? Does the patient need a medical certificate?
Complications.What can go wrong during and after the operation?
Prognosis.What is the success rate of the surgical procedure, and for how long will the benefits of the operation last?
Various Disciplines in the Field of Surgery
The American College of Surgeons recognizes multiple surgical specialties [1]. As you consider the type of specialty that is best for you, it’s helpful to review your available options.
General surgery is performed by surgeons trained to manage surgical procedures covering almost any area of the body. Within general surgery are subspecialties that include the following:
Colon and Rectal Surgery is also known as proctology. The focus is on the diagnosis and treatment of disorders such as inflammatory bowel disease, pelvic floor dysfunction and colorectal cancer.
Ear, nose and throat surgery, also known as otolaryngology – diseases and disorders affecting the ears and structures within the respiratory system.
Maxillofacial and Oral surgery also includes dental surgery – treatment for patients with face, facial skeleton, mouth and related organs injuries, diseases and disorders.
Obstetrics and gynecology – medical and surgical care for pregnant patients, including the development of the fetus and disorders of female reproductive organs.
Ophthalmic surgery – diseases and disorders of the eye, vision, and contents of the eye socket.
Orthopedic surgery – anything having to do with the musculoskeletal system including bones, muscles, and joints. Subspecialties of orthopedics are:
Foot and ankle
Hand – includes upper extremities.
Joint replacement – mostly the hips and knees, but can include the ankles and shoulders.
Oncology – treatment for benign and malignant tumors of the musculoskeletal system.
Pediatrics – orthopedic conditions in children.
Spine – manages the care and treatment of back problems.
Sports – focuses on patients who are athletes and individuals suffering from athletic injuries.
Trauma orthopedics is a growing field. Patients are individuals with critical or multiple injuries to the musculoskeletal system.
Pediatric surgery – disorders for individuals still considered children, including teenagers. There are multiple subspecialties within this area.
Neonatal – newborn care.
Prenatal – fetal care.
Trauma – Because children take lots of risks and end up hurting themselves, pediatric surgeons frequently face situations involving traumatic injuries sustained by children.
Oncology – malignant tumors and benign growths.
Plastic and maxillofacial surgery – cosmetic procedures and the repair of body parts after the loss of tissue such as an ear. Thorough knowledge of the musculoskeletal system is critical.
Thoracic surgery – anything in the chest area, but primarily the heart and lungs.
Urology – manages benign and malignant medical and surgical disorders of the adrenal gland and the genitourinary system for both males and females.
Vascular surgery – treats diseases impacting the arteries and veins throughout the body. Hardening of the arteries may be the most common problem that vascular surgeons treat.
Types of Surgery
Once you become a surgeon, you may be called upon to perform one or all of the following types of procedures.
Open surgery is when a surgeon makes an incision with a scalpel, inserts instruments into the opening and performs surgery. An example of open surgery is a surgeon making an incision with a steel scalpel in the abdominal skin to perform a gastric operation.
Aspirationis a type of biopsy procedure where fluid and diseased tissue are removed by a needle for laboratory examination. An example of this is a breast biopsy where the tissue removed is sent to a lab to determine if it is cancerous.
Cryosurgery is a minimally invasive treatment where diseased tissue is destroyed by freezing it. Skin tumors, skin tags, and even freckles can be removed by this method of surgery.
Electrosurgery uses electrical instruments operating on high-frequency electric currents. Electric currents can harden tissue, or destroy it. In essence, a surgeon “burns” away diseased tissue, or growths, or make surgical incisions while the electric current seals off blood vessels at the same time, thus minimizing bleeding.
Laser surgery utilizes a laser beam to make bloodless cuts in tissue or to remove surface lesions. Lasers can be used for eye surgery, removal of skin marks and small tumors.
Scope surgery is minimally invasive since it does not involve slitting open the body as a surgeon does in open surgery. Some common scope surgeries include laparoscopy, endoscopy, and colonoscopy.
Shockwaves is a noninvasive surgical technique where soundwaves are used to break apart kidney stones. However, the sound, or shockwaves come from outside the body. Currently it is considered the surgery of choice to break apart large kidney stones.
Ultrasonic scalpels use soundwaves to make surgical incisions that minimize This type of surgery is used when extreme precision is needed to remove small and delicate tissues, but can also be used for large tissue removal.
Post-surgical Discomforts and Complications
No matter how minor the surgery, almost all patients experience a period of discomfort during the healing process. Although every patient heals differently, most discomfort improves daily and ultimately disappears. Some of the most common discomforts include:
Constipation and gas (flatulence).
Nausea and vomiting from general anesthesia.
Restlessness and sleeplessness.
Soreness, pain, and swelling around the incision site.
Sore throat (caused by the tube placed in the windpipe for breathing during surgery).
Thirst.
No operation is routine. All surgeries carry with them some inherent risk because most surgeries invade the body. Risk can result in complications. Complications common to all surgeries are excessive bleeding during or after an operation and infection of surgical wounds. Others are:
Delayed healing and non-healing wounds. An example of this is a broken bone taking a very long time to heal, or perhaps it will not grow together at all.
A hemorrhage occurs when there is rapid blood loss from the site of surgery. This may lead to shock, so it must be treated quickly.
Loss of function. Sometimes a patient will be unable to perform one or more tasks or activities after the operation that were possible before the surgery.
Lung (pulmonary) complications. This complication is monitored for the first 48 hours after surgery. Sometimes deep breathing and coughing exercises are mandated for the patient to minimize the risk. The most common symptoms include wheezing, chest pain, fever, and cough.
Neurological complications.These may manifest as the loss of individual senses such as vision, feeling in a specific area, or control of a voluntary muscle.
Reaction to anesthesia. Although rare, patients can experience mild to severe allergic reactions to anesthetics.
Rejection. An example of this is the rejection of a transplanted organ such as a kidney.
Shock. Shock is created by excessive bleeding, wound infection, brain injury or metabolic problem. Immediate treatment is required.
Sinuses and fistulas. These are small canals and holes which can result from surgery.
Urinary retention. Temporary urine retention, or the inability to empty the bladder, may occur after surgery due to anesthesia.
Wound infection. When bacteria enter the site of surgery, an infection can result that delays healing. In some cases, wound infections can spread to nearby organs or tissue, or to distant areas through the bloodstream.
Other complications are more external. They may not impair function, present life-threatening situations or interfere with activities of daily living. But they can lower self-esteem and self-confidence because they can be obvious and mar external aesthetics. For a patient these conditions can be all-consuming and surgeons must be prepared to manage the emotional implications. External complications include:
Over exuberant healing
Keloid – a growth-like scar of a surgical wound.
Scarring – usually harder than the adjacent tissue and often cosmetically not pleasing.
Pigmentation and loss of normal pigmentation – discoloration or loss of normal coloring to the area.
Frontiers of Surgery
Medical science is always evolving. Doctors and researchers are continually looking for ways to minimize risk, pain, infection and healing time to patients. There are two types of surgery on the leading edge of medicine.
Robotic surgery. With the use of a camera and mechanical arms with surgical instruments attached to them, a surgeon can operate by sitting at a computer console. The console provides the surgeon with a magnified, three-dimensional view of the surgical site from which she or he controls the movement of the mechanical arms. The advantages of this technology include fewer complications, quicker recovery and smaller, perhaps less visible scars. As robotic surgery is refined, it’s possible that surgery can be performed on a patient who is a long distance away, including operations on astronauts in space or soldiers in the battlefield.
Healthcare Informatics, formerly known as The Institute for Health Technology Transformation (iHT2) commissioned a video featuring Intuitive Surgical’s da Vinci Arm device. Dr. David Samadi of Mount Sinai School of Medicine explains the arm and gives his thoughts on the future of robotic surgery.
Tissue engineering/regenerative medicine. Although regenerative medicine does not yet play a significant role in treatment, it has the potential of transforming how surgery is approached. According to the National Institute of Biomedical Imaging and Bioengineering, the goal of tissue engineering is to develop,“biological substitutes that restore, maintain, or improve tissue function.” [2]. They developed a two-minute video on tissue engineering which you can see here:
Medical scientists can already grow specific types of tissue from the patient’s own cells, thereby avoiding the risk of rejection. The FDA has approved the use of artificial skin and cartilage, although their use in patients is still limited. The growing of an organ, such as a kidney from the patient’s own cells, appears to be just around the corner.
A mini bio-engineered human liver that can be implanted into mice. (Source: Sangeeta Bhatia, MIT)
The History of Surgery
The Egyptians practiced surgery as early as 1600 B.C. Papyrus scrolls vividly describe the splinting of fractures, the care of wounds, the drainage of abscesses, etc.
Hippocrates(400 B.C.), commonly described as “the father of medicine,” wrote books on surgery, including the treatment of head injuries. TheHippocratic Oathis a pledge some medical students make when they become doctors and is commonly believed to include the phrase, “first, do no harm.”
As surprising as it sounds, during the Middle Ages, surgery was mainly performed by barbers as part of their duties. They aided monks, who, at that time were considered the primary practitioners of medicine. But a Papal decree forbade monks to spill blood on themselves, so surgery was performed by the barbers instead. Over time surgery was claimed by scientific medicine in the 16th to 18th centuries.
John Hunter, a Scottish surgeon (1728-1793), applied experimental methods in surgery. He taught his students that a surgical operation was the last resort and an admission that other methods had failed.
Two seemingly impossible situations presented stumbling blocks in the field of surgery. One was the excruciating pain associated with surgical interventions. The other was the almost inevitable wound infections occurring after surgery, especially surgery to the abdomen, chest, and skull. Most of these were fatal.
In the 1840’s, English surgeonJoseph Listerovercame the problem of intense pain through the use of anesthesia. In the 1860s, he introduced principles of surgery which significantly reduced infection.
The 20th century saw a rapid expansion and refinement in anesthetic technique, anesthetic agents and machines, sterility and asepsis, and the discovery of antibiotics. Each advancement allowed surgery to expand into many sub-surgical disciplines. With them came new, safer and less invasive surgical techniques which have become the standard surgical practices and procedures of today.
The development of the heart-lung machine made safe surgery to the heart possible – culminating in the first successful human heart transplant in 1967 byProfessor Christiaan Barnard, a South African heart surgeon.
Since 1967, there have been many additional contributions in surgical history, particularly ones that lead to its newest frontiers.
What is the best material to practice your suturing skills on?
Although silicon skin is helpful and convenient for the practice of suturing, it doesn’t always behave like real skin. It looks authentic, but the feel, touch and handling characteristics are imprecise if you’re looking for a genuine experience. That’s why buying high quality silicon skin is crucial if your objective is perfecting your suturing technique.
When you are preparing to start suturing on real patients in a clinical setting you want to experience some form of realism. Our philosophy and recommendation to teachers and students are simple. First master the various basic suturing patterns on a suture pad or other type of synthetic skin.
Once you have mastered your technique, go to a butcher shop or the butchery department of your grocery store and buy a suitable piece of meat with the skin attached. (Ask your butcher for advice. Pork shank, chicken or turkey with skin will serve the purpose well.) Practicing on a cut of meat is the closest approximation of human skin and muscle that you can get in a medical education setting.
Believe me – real meat from the butcher will offer you the highest level of realism possible short of suturing on real people in a clinical setting.
That said, you don’t initially need super realism to practice your suturing skills. A suture pad is more than adequate for your first practice runs. After that, strive for the most realistic option; meat from your butcher.
Master surgical suturing skills
You will find a very specific, easy and effective system of learning suturing skills in The Apprentice Doctor’sSuturing Kit and Course. Using the suturing course, you’ll master basic surgical knot tying after which you are ready to start practicing the 11 basic suturing techniques.
For those students who own some suturing tools but lack silicon skin, and find replacing cuts of meat too pricey, you may find The Apprentice Doctor’sSuture Pad/Suturing Model for Practicing Suturing an ideal compromise. Its realistic, durable design with veins, skin, fat and muscle layers is perfect for medical students, veterinarians, nurses, and emergency personal to practice and perfect suturing and laceration repair.
Both kits will allow you to become confident performing suturing procedures. You’ll feel calmer and more in control when suturing in high stress environments.
I really want to become a Doctor – Is there anything I can do straight away?
IMPORTANT! A major website update has been made. Any issues, notify us instantly by pressing the "Quick Help" button and leaving a short description of what you experienced.
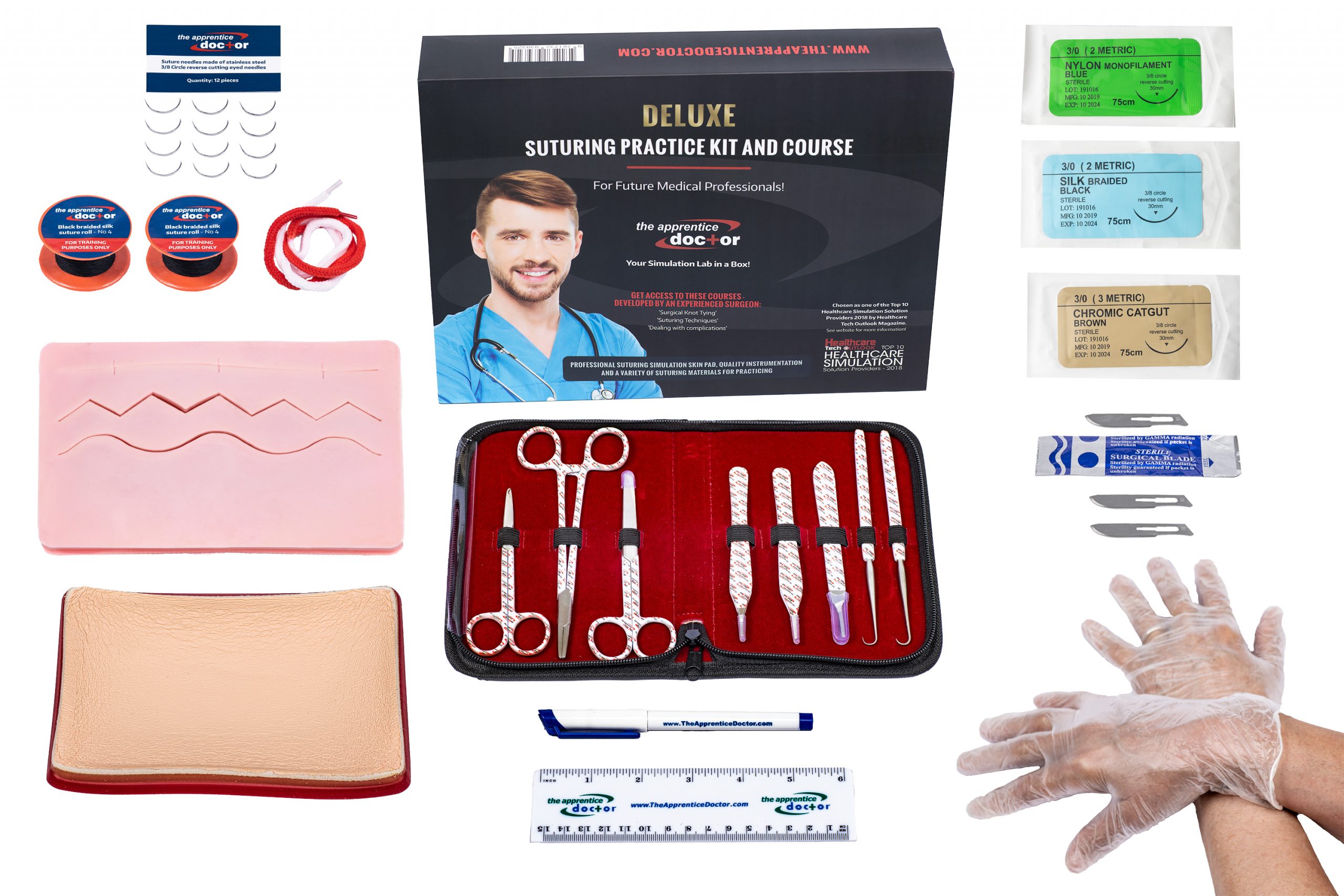

 Story at a Glance
Story at a Glance In the field of medicine, continuing education is mandatory. Trauma surgeons must stay abreast of advancements in surgical techniques. The better the methods and tools, the less risk there is to patients. Educational content varies depending on a doctor’s specialty. However, the surgical material is more complicated. Minimal requirements for continuing education are ten hours of participation in an accredited continuing medical education program. The
In the field of medicine, continuing education is mandatory. Trauma surgeons must stay abreast of advancements in surgical techniques. The better the methods and tools, the less risk there is to patients. Educational content varies depending on a doctor’s specialty. However, the surgical material is more complicated. Minimal requirements for continuing education are ten hours of participation in an accredited continuing medical education program. The





 Are you a little uncomfortable interacting with people all the time? Feeling drained of energy when talking with others without periods of quiet could mean you’re introverted. That means you need time away from lots of activity in order to recharge yourself. Extroverts, on the other hand, gain vitality from being around people. That’s how they rejuvenate themselves. The good news is that healthcare needs both types of personalities.
Are you a little uncomfortable interacting with people all the time? Feeling drained of energy when talking with others without periods of quiet could mean you’re introverted. That means you need time away from lots of activity in order to recharge yourself. Extroverts, on the other hand, gain vitality from being around people. That’s how they rejuvenate themselves. The good news is that healthcare needs both types of personalities. Job Responsibilities: Lab technicians, or MLTs, work with integrated systems and perform mechanical or diagnostic tests in medical laboratories. Some MLTs work independently while others prefer to work in companies where they’re part of more extensive teams of professionals.
Job Responsibilities: Lab technicians, or MLTs, work with integrated systems and perform mechanical or diagnostic tests in medical laboratories. Some MLTs work independently while others prefer to work in companies where they’re part of more extensive teams of professionals.
 Job Responsibilities: Professionals who study the minute structures of biological material and determine how they are structurally and functionally related are called histotechnicians. The field encompasses how biochemistry, molecular biology, and physiology interact with disease processes. Like other MLT specialties, you’ll be studying and analyzing samples and reporting data to researchers, doctors, and scientists.
Job Responsibilities: Professionals who study the minute structures of biological material and determine how they are structurally and functionally related are called histotechnicians. The field encompasses how biochemistry, molecular biology, and physiology interact with disease processes. Like other MLT specialties, you’ll be studying and analyzing samples and reporting data to researchers, doctors, and scientists. Job responsibilities: First and foremost, a PA helps a pathologist prepare and diagnose tissue, blood and other specimens in a sterile laboratory. Depending upon the work environment, as a PA you might also examine corpses to determine a cause of death. Tasks could include collecting and dissecting postmortem specimens, conducting various tests on samples, taking diagnostic images, and recording your findings. From time-to-time some PAs may be asked to train colleagues or assist with autopsies, which does require some social interaction. However, most responsibilities are lab-based and can be performed independently.
Job responsibilities: First and foremost, a PA helps a pathologist prepare and diagnose tissue, blood and other specimens in a sterile laboratory. Depending upon the work environment, as a PA you might also examine corpses to determine a cause of death. Tasks could include collecting and dissecting postmortem specimens, conducting various tests on samples, taking diagnostic images, and recording your findings. From time-to-time some PAs may be asked to train colleagues or assist with autopsies, which does require some social interaction. However, most responsibilities are lab-based and can be performed independently.
 Job responsibilities: If you enjoy working with machinery, but also being a member of a care team with indirect responsibility for patients, then a career as an anesthesia technician may be right for you.
Job responsibilities: If you enjoy working with machinery, but also being a member of a care team with indirect responsibility for patients, then a career as an anesthesia technician may be right for you. Job Responsibilities: Although not specifically a medical lab job, radiation protection technicians provide a valuable service to overall public health. RPTs are also referred to as nuclear monitoring technicians or hazardous materials removal workers. As the titles imply, RPTs track radiation levels. They also expose leaks or potential hazards and then remove them. As an RPT you may even find yourself organizing evacuations of contaminated areas. The type and seriousness of the emergency determine the protocol followed. Some RPTS specialize in decontamination, emergency response or storage, and disposal. Or you’ll analyze environmental samples to determine levels of contamination.
Job Responsibilities: Although not specifically a medical lab job, radiation protection technicians provide a valuable service to overall public health. RPTs are also referred to as nuclear monitoring technicians or hazardous materials removal workers. As the titles imply, RPTs track radiation levels. They also expose leaks or potential hazards and then remove them. As an RPT you may even find yourself organizing evacuations of contaminated areas. The type and seriousness of the emergency determine the protocol followed. Some RPTS specialize in decontamination, emergency response or storage, and disposal. Or you’ll analyze environmental samples to determine levels of contamination.













 Today we present an interview with Leann Williams, a surgical technologist and surgical technologist educator from Tucson, Arizona.
Today we present an interview with Leann Williams, a surgical technologist and surgical technologist educator from Tucson, Arizona.
 What does a surgical assistant do?
What does a surgical assistant do?
 Surgical technologists are important members of surgical teams, especially since technologists are responsible for many preparatory tasks relating to surgeries. For example, you may be asked to prepare an operating room. This can range from setting up trays of instruments in a sterile field to preparing patients for surgery. Because you’ll know how medical equipment works you may be required to ensure all surgical machines are working properly. You will be familiar with these tasks since they are all part of a surgical technology education.
Surgical technologists are important members of surgical teams, especially since technologists are responsible for many preparatory tasks relating to surgeries. For example, you may be asked to prepare an operating room. This can range from setting up trays of instruments in a sterile field to preparing patients for surgery. Because you’ll know how medical equipment works you may be required to ensure all surgical machines are working properly. You will be familiar with these tasks since they are all part of a surgical technology education.